- Main article: Psychological aspect of breast feeding
- Main article: Psychological aspects of weaning

{kind=link}
A breastfeeding infant
Breastfeeding is the process of a woman feeding an infant or young child with milk from her breasts, usually directly from the nipples. Babies have a sucking urge that enables them to take in the milk, provided there is a good latch, a normal frenulum, and a milk supply.
Breast milk has been shown to be best for feeding a child (assuming the mother does not have any serious transmissible infections.) Some mothers do not breastfeed their children, either for personal or medical reasons. Some diseases, such as HIV and HTLV-1, may be passed through the breast milk, and may therefore preclude breastfeeding in some cases. Some medicines may also transfer through breast milk. However, most medicines are transferred in very small amounts and are considered safe to take during breastfeeding. Therefore most women are not precluded from breastfeeding, and most doctors and governments promote the practice. Still, many medications are labelled as unsafe for use while breastfeeding, and the breastfeeding mother and her physician must carefully weigh the risks and benefits.
Assessment |
Biopsychology |
Comparative |
Cognitive |
Developmental |
Language |
Individual differences |
Personality |
Philosophy |
Social |
Methods |
Statistics |
Clinical |
Educational |
Industrial |
Professional items |
World psychology |
Clinical: Approaches · Group therapy · Techniques · Types of problem · Areas of specialism · Taxonomies · Therapeutic issues · Modes of delivery · Model translation project · Personal experiences ·
Many governmental strategies and international initiatives have promoted breastfeeding as the best method of feeding a child in his or her first year and beyond. So do the World Health Organization (WHO),[1] the American Academy of Pediatrics (AAP),[2] and many others.
Beginning lactation
.png){kind=link}
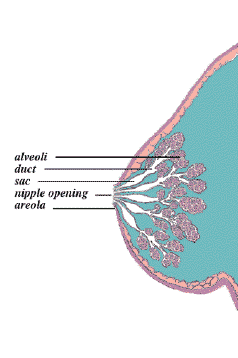
When the baby sucks, a hormone called oxytocin starts the milk flowing from the alveoli, through the ducts (milk canals) into the sacs (milk pools) behind the areola and finally into the baby's mouth
Main article: Breast milk
Throughout the last two trimesters of pregnancy a woman's body produces hormones which stimulate the growth of the milk duct system in the breasts:
- Progesterone -- influences the growth in size of alveoli and lobes. Progesterone levels drop along with oestrogen levels after birth, triggering the onset of copious milk secretion.[3]
- Oestrogen -- stimulates the ductule system to grow and become specific. Estrogen levels drop at delivery and remain low for the first several months of breastfeeding.[3] (This is also why it is recommended that breastfeeding moms avoid oestrogen-based birth control methods while they are planning to breastfeed. A spike in oestrogen levels compromises a mother's milk supply level.)
- Follicle stimulating hormone (FSH)
- Luteinizing hormone (LH)
- Prolactin -- contributes to the accelerated growth of the alveoli during pregnancy [4].
- Oxytocin -- contracts the smooth muscle of the uterus during birth, after birth, and during orgasm. After birth, oxytocin contracts the smooth muscle layer of band-like cells surrounding the alveoli to squeeze the newly-produced milk into the duct system. Oxytocin is necessary for a let-down, or milk ejection reflex, to occur. [4]
- Human placental lactogen (HPL) -- HPL is released in large amounts by the placenta during pregnancy (beginning in the second month) that appears to be instrumental in breast, nipple, and areolar growth before birth. [4]
By the fifth or sixth month of pregnancy, the breasts are sufficiently developed to produce milk (although it is also possible to induce lactation as described in a later section).
During the latter part of pregnancy, the woman's breasts enter into the Lactogenesis I stage, where the breasts are making colostrum (a thick, sometimes yellowish fluid), but high levels of progesterone inhibit most milk secretion and keep the volume “turned down”. It is considered medically normal for a pregnant woman to leak colostrum before her baby's birth, and also normal not to leak at all. Neither situation is an indicator of future milk production levels in the mother.
At birth, the delivery of the placenta results in a sudden drop in progesterone/oestrogen/HPL levels. This abrupt withdrawal of progesterone in the presence of high prolactin levels cues Lactogenesis II (copious milk production).
Prolactin blood levels rise when the breast is stimulated, and peak around 45 minutes later. They return to pre-breastfeeding levels about three hours afterwards. The release of prolactin triggers the cells in the alveoli to create milk. Some research [5] indicates that prolactin in milk is higher at times of higher milk production, and that the highest levels tend to occur between 2 a.m. and 6 a.m.
Other hormones (insulin, thyroxine, cortisol) are also involved, but their roles are not yet well understood. Although biochemical markers indicate that Lactogenesis II commences approximately 30-40 hours after birth, mothers do not typically begin feeling increased breast fullness (the sensation of milk "coming in") until 50-73 hours (2-3 days) after birth.
The colostrum is the first milk the baby receives; it contains higher amounts of white blood cells and antibodies than mature milk, and is especially high in immunoglobulin A (IgA), which coats the lining of babies' immature intestines, helping to prevent germs from invading baby's system. Secretory IgA also works to help prevent food allergies. [6]
After a baby has been nursing for 3-4 days, the colostrum in the breast slowly begins the process of changing into mature breast milk over the next two weeks. [3]
During pregnancy and the first few days postpartum, milk supply is hormonally driven. This is the endocrine control system. After milk supply has been more firmly established, Lactogenesis III begins - the autocrine (or local) control system.
At this stage, milk production follows the law of supply and demand: The more milk removed from the breast, the more milk the breast will produce. Thus milk supply is strongly influenced by how often the baby feeds and well it is able to transfer milk out of the breast. "Low supply" can often be traced to:
- not feeding or pumping often enough,
- inability of the infant to transfer milk effectively caused by, among other things:
- jaw or mouth structure deficits
- poor latching technique
- inadequate calorie intake or malnutrition of the mother
- a metabolic or digestive inability in the infant, rendering it unable to utilize the milk it receives.
Research on mothers who express their milk [7] [8] indicate that for most women the more times per day a mother expresses her milk, the more milk she produces. Ongoing research [9] shows that more fully draining the breasts also increases the rate of milk production.
The production, secretion and ejection of milk is called lactation. Most breastfeeding experts recommend at least one feeding every two to three hours to maintain the milk supply. For most women, a target of eight (8) nursing sessions/pumping sessions per 24 hours seems to keep a milk supply high not only during the early months of lactation, but especially past the fourth month. [10] It is not at all uncommon for newborn infants to nurse far in excess of this amount: 10 to 12 nursing sessions per 24 hours is the comparative norm, while some may even nurse 18 times in the same time frame.
The exact properties of breast milk are not entirely understood, but the nutrient content of mature milk is relatively consistent and draws its ingredients from the mother's food supply and the nutrients in her bloodstream at the time of feeding. If that supply is inadequate, content is obtained from the mother's bodily stores. (Some studies estimate that a woman burns an extra 500 calories per day simply producing milk for her offspring.) The exact composition of breast milk varies from day to day, and even hour to hour, depending on both the manner in which the baby nurses and the mother's food consumption and environment, so the ratio of water to fat fluctuates. Foremilk, the milk released at the beginning of a feed, is watery, low in fat and high in carbohydrates compared with the creamier hindmilk which is released as the feed progresses. There is no sharp distinction between foremilk and hindmilk – the change is very gradual. Research from Peter Hartmann's group tells us that fat content of the milk is primarily determined by the emptiness of the breast -- the less milk in the breast, the higher the fat content. The breast can never be truly "emptied" since milk production is continuous.
The let-down reflex
The let-down reflex, also known as the milk ejection reflex, is caused by the release of the hormone, oxytocin. Oxytocin stimulates the muscles of the breast to squeeze out the milk. Breastfeeding mothers describe the sensation differently, with some feeling a slight tingling, some feeling immense amounts of pressure and slight pain/discomfort, and still others not feeling anything different.
The reflex is not always consistent, especially at first. The thought of nursing or the sound of any baby can stimulate the let-down reflex, causing unwanted leakage, or both breasts give out milk when one infant is feeding. However, this and other problems often settle after two weeks of feeding. If the mother is in a stressed or anxious state of mind this can cause difficulties with breastfeeding.
Causes of a poor let-down reflex:
- Sore or cracked nipples
- Separation from the infant
- A history of breast surgery
If a mother has trouble breastfeeding she can try different methods of assisting the let-down reflex. These include:
- Feeding in a familiar and comfortable location
- Massage of the breast or back
- Warming the breast with a cloth or shower
After-Pains
The surge of oxytocin for triggering milk let-down also causes the uterus to subinvolute (contract down). Subsequently, during breastfeeding mothers can feel uterine contractions (pain ranging from period-like cramps to strong labour-like contractions). Afterpains can be more severe with second and subsequent babies. [11]
Benefits
The benefits of breastfeeding are both physical and psychological for both mother and child. Nutrients and antibodies are passed to the baby while hormones are released into the mother's system. The bond between baby and mother can also be strengthened during breastfeeding.
Benefits for the infant
Breastmilk, when fed directly from the breast, is immediately available with no wait and is at body temperature.
Breast fed babies have a decreased risk for several infant conditions including Sudden Infant Death Syndrome(SIDS). The sucking technique required of the infant encourages the proper development of both the teeth and other speech organs.
The many health benefits of breastfeeding have been well documented. According to the American Academy of Pediatrics policy statement, "Extensive research, especially in recent years, documents diverse and compelling advantages to infants, mothers, families, and society from breastfeeding and the use of human milk for infant feeding. These include health, nutritional, immunologic, developmental, psychological, social, economic, and environmental benefits.
Breast milk helps to lower the risk of or protect against:
- Diabetes
- Gastroenteritis
- Diarrhoea
- Asthma
- Allergies
- Urinary tract infection
- Chest infection and wheezing
- Ear infection
- Obesity
Benefits for the mother
Breastfeeding also benefits the mother. Breastfeeding releases hormones that have been found to relax the mother and cause her to experience nurturing feelings toward her infant. Breastfeeding as soon as possible after giving birth increases levels of oxytocin which encourages the uterus to contract more quickly. This helps to decrease bleeding after the birth. Breastfeeding can also help the mother to return to her previous weight as the fat accumulated during pregnancy is used in milk production. Frequent and exclusive breastfeeding delays the return of menstruation and fertility known as lactational amenorrhoea. This allows for improved iron stores and the possibility of natural child spacing. Breastfeeding mothers experience improved bone re-mineralisation after the birth, and a reduced risk for both ovarian and breast cancer both before and after menopause.
Bonding
The maternal bond is strengthened through breastfeeding, with the hormonal releases strengthening the mother's nurturing feelings towards the child. Strengthening the maternal bond is very important as studies show that up to 80% of mothers suffer from some form of postpartum depression, though most cases are very mild. The father can support the mother in a variety of ways and is an important factor in successful breastfeeding. This support can also help to establish the paternal bond in fathers.
Breastfeeding can also greatly affect the personal relationship between the partner and the child. While some fathers may feel left out when the mother is feeding the baby, others may see the whole process as a chance to bond as a family. Breastfeeding, possibly alongside birth-related health problems, takes a lot of time. This may add pressure to the father and the family, because the partner has to care for the mother and also perform tasks she would otherwise do. However, as fathers are often very willing to give this support, this pressure can help to strengthen family bonds.
When looking after the child while the mother is away, an alternative caregiver may feed the child using expressed breast milk (EBM). Sometimes this may be impractical as the mother must produce and store enough milk to feed the child for the duration of her absence. If the two caregivers are separated, feeding the breast milk may also be awkward. These two situations may prompt the caregivers to use an alternative feeding method for the child either temporarily or permanently. However, a variety of breast pumps now on the market, both for sale and for rent, make it possible for working mothers to exclusively breastfeed their babies for as long as they wish.
Recommendations and research
"A vast majority of mothers can and should breastfeed, just as vast majority of infants can and should be breastfed. Only under exceptional circumstances can a mother's milk be considered as unsuitable for her infant. For those few health situations where infants cannot, or should not, be breastfed, the choice of the best alternative is: expressed milk from the infant's own mother, breast milk from a healthy wet-nurse or a human-milk bank, or a breast milk substitute fed with a cup, which is a safer method than a feeding bottle or a teat; depends on individual circumstances. Infants who are not breastfed, for whatever reason, should receive special attention from the health and social welfare system since they constitute a risk group." (World Health Organization, "Global strategy for infant and young child feeding," section titled "EXERCISING OTHER FEEDING OPTIONS" 24 November 2001)http://www.who.int/gb/ebwha/pdf_files/EB109/eeb10912.pdf
Difficulties with breastfeeding
It is not uncommon for a mother and child to have difficulties breastfeeding in the beginning, but most of these problems resolve in the early weeks.
Small percentages (between 2 & 3%) of women are unable to provide a full day's calories. It is not known what causes insufficient milk supply, but extended separation at birth, insufficient glandular tissue, and Polycystic Ovary Syndrome (PCOS) are all known culprits. Even among this small group, it is feasible to continue breastfeeding while supplementing with donated breastmilk or artificial baby milk. Many of these mothers breastfeed exclusively by using thin tubing taped to the breast to deliver the supplementary food. This is called a supplementary nursing system, or SNS.
While some may find it too problematic or choose not to attempt or continue breastfeeding for personal reasons, most women who have initial difficulties can go on to breastfeed successfully.
Breast refusal
Though babies have a natural sucking reflex, they still have to learn how to feed and may occasionally resist feeding from the breast. To establish breastfeeding firmly, it is important for the baby to be put to the breast soon after birth so that the baby is accustomed to feeding from the breast from the very beginning. The AAP policy on breastfeeding says: Delay weighing, measuring, bathing, needle-sticks, and eye prophylaxis until after the first feeding is completed.
Causes of breast refusal include:
- Formula feeding, sometimes without the knowledge of the mother.
- The use of artificial teats (nipples) or dummies leading to "nipple confusion"
- Poor feeding technique
- Over-handling after birth
- Thrush in the baby's mouth [1] [2]
- Distractions or interruptions during feeds
- Long separations from the mother
- Breathing difficulties, often caused by a common cold [3]
- Swallowing difficulties, sometimes the painful result of ear or throat infections
- Pain from surgery (most commonly circumcision), blood tests, vaccinations, and other procedures commonly done without anaesthesia [4] [5]
In later stages teething could be perceived by the mother as a hindrance to breastfeeding. While it is seen by some as a good time to wean the infant, teething difficulties can usually be overcome.
Medical conditions of the infant
Reasons for the inhibition of an infant to feed include:
- Difficulties latching onto the breast
- Poor sucking reflex
- Poor stamina
- Medical conditions such as cleft palate
- Hypoglycemia or hyperglycemia
- Hypotonia, or "low-tone" infant disorder
Premature babies can have difficulties if their sucking reflex is still underdeveloped and if they tire during feeds.
For many sucking related feeding difficulties, the infant can receive proper nutrition by use of a Haberman Feeder, a special bottle with a carefully designed nipple that simulates breastfeeding.
Medical conditions of the mother
Many women with previous surgeries, abscesses and cancer can breastfeed successfully. However, damage to the breast tissue can cause problems or prevent manageable breastfeeding for women with history of breast surgery or infection. Cancer (particularly breast cancer) and chemotherapy treatments have also been shown to cause difficulties. Infectious diseases such as HIV, AIDS, or active, untreated tuberculosis can be passed onto the infant. A HIV-positive mother breastfeeding an infant can, in some countries, be investigated for child abuse – a 1998 case in the U.S. resulted in the HIV-positive mother being reported to social services for her continued breastfeeding and non-treatment of the child for HIV [6]. The presence of herpes lesions on the breast is also contraindicative to breastfeeding.
Mastitis is inflammation of the breasts caused by the blocking of the milk ducts. Mastitis cause painful areas on the breasts or nipples and may lead to a fever or flu-like symptoms. It is not necessary to wean a nursling simply because of mastitis; in fact, nursing is the most effective way to remove the blockage and alleviate the symptoms, and is not harmful to the baby. Sudden weaning can cause or exacerbate mastitis symptoms.
When breastfeeding may be harmful to the infant
Breastfeeding may be harmful to the infant if the mother:
- has HIV or active tuberculosis [citation needed]
- is taking certain medications that suppress the immune system
- is taking certain medications which may be passed onto the child through the milk and are found to be harmful. However, the vast majority of medications are compatible with breastfeeding.
- has had excessive exposure to heavy metals such as mercury
- uses potentially harmful substances such as cocaine, heroin and amphetamines. Substances such as caffeine, tobacco, and alcohol, while possibly harmful to the nursling if consumed in large quantities, are safe to use in moderation while breastfeeding (see below).
Health and diet
Since the nutritional requirements of the baby must be satisfied solely by the breast milk in exclusive breastfeeding it is important for the mother to maintain a healthy lifestyle, especially her diet. If the baby is large and grows quickly, the fat stores gained by the mother during pregnancy can be quickly depleted, and she may have trouble eating well enough to keep developing sufficient milk. The diet usually involves a high calorie, high nutrition diet which follows on from that in pregnancy. The Subcommittee on Nutrition during Lactation advises approximately 1500–1800 calories per day [7]. While mothers in famine conditions can produce milk with highly nutritional content, a malnourished mother may produce milk with decreased levels of vitamins A, D, B6 and B12. She may also have a lower supply than well-fed mothers [8].
There are no foods which are absolutely contraindicated during lactation, although a baby may show sensitivity to particular foods in the mother's diet. Some breastfeeding advisers suggest mothers avoid certain gas producing food, such as beans, if the baby starts to develop colic or gas.[citation needed]
Breastfeeding mothers must use caution if they smoke and therefore consume nicotine. Heavy use of cigarettes by the mother (more than 20 per day) has been shown to reduce the mother's milk supply and cause vomiting, diarrhoea, rapid heart rate, and restlessness in breastfeeding infants. Research is ongoing to determine whether the benefits of breastfeeding out-weigh the potential harm of nicotine in breast milk. Sudden Infant Death Syndrome (SIDS) is more common in babies exposed to a smoky environment [9]. Breastfeeding mothers who smoke are counselled not to do so during or immediately before feeding their child. They are encouraged to seek advice to help them reduce their nicotine intake or quit.
Heavy alcohol consumption is known to harm the infant, causing problems with the development of motor skills and decreasing the speed of weight gain. There is no consensus on how much alcohol may be consumed safely, but it is generally agreed that small amounts of alcohol may be occasionally consumed by a breastfeeding mother. However, some believe that a single daily glass of wine is enough to cause distress, with levels of alcohol in breast milk peaking 30 to 90 minutes after one drink of moderate alcoholic content. Considering the known dangers of alcohol exposure to the developing fetus, many medical professionals believe it is preferable to err on the side of caution and have breastfeeding women restrict or eliminate their alcoholic intake.
Excessive caffeine consumption by the mother can cause irritability, sleeplessness, nervousness and increased feeding in the breastfed infant. Moderate use (one to two cups per day) usually produces no effect. Breastfeeding mothers are advised to avoid or restrict caffeine intake.
Cannabis is listed by the American Association of Pediatrics as a compound that transfers into human breast milk.[10] This is based on research which demonstrated that certain compounds in marijuana have a very long half-life. Cannabis exposure via the mother's milk during the first month postpartum appears to be associated with a decrease in infant motor development at one year of age.
Signs of a Well-Fed Newborn
- At least 8 breastfeeds every 24 hours (10-12 in 24 hours is more common in newborns)
- Obviously swallowing during the feeds
- Seems happily satisfied after the feeds
- Baby is allowed to determine the length of the feeding, which may be 10 to 20 minutes or longer, on one breast or two.
- No meconium faeces by Day-5 ("The normal breastmilk stool is pasty to watery, mustard coloured, and usually has little odour. However, bowel movements may vary considerably from this description. They may be green or orange, may contain curds or mucus, or may resemble shaving cream in consistency (from air bubbles). The variations in colour do not mean something is wrong. A baby who is breastfeeding only, and is starting to have bowel movements that are becoming lighter by day 3 of life, is doing well." (Handout #4. Is My Baby Getting Enough Milk? Revised January 2005, Written by Jack Newman, MD, FRCPC. © 2005)
- At least three soiled diapers in 24 hours, with stools at least the size of a US quarter.
- Five (5) to six (6) wet disposable diapers in 24 hours, or six (6) to eight (8) wet cloth diapers in 24 hours. (After one week of age) A good comparison tool for an adequately "wet" diaper is to pour three US Tablespoons of water into a dry diaper.
- Baby should be gaining at least 4-7 ounces per week after the fourth day of life. (Most infants lose 7 to 10 percent of their birth weight during the first week of life, and regain it again by the second week.)
- Thereafter gaining 100g-200g per week.
Baby's Age Average Weight Gain 0-4 months: 170 grams per week † 4-6 months: 113-142 grams per week 6-12 months: ‡ 57-113 grams per week † It is acceptable for some babies to gain 4-5 ounces (113-142 grams) per week.
‡ The average breastfed baby doubles birth weight in 5-6 months. By one year, the typical breastfed baby will weigh about 2 1/2 times birth weight. By two years, differences in weight gain and growth between breastfed and formula-fed babies are no longer evident.
Source: Mohrbacher N and Stock J. The Breastfeeding Answer Book, Third Revised ed. Schaumburg, Illinois: La Leche League International, 2003, p. 148-149.
Signs of an Underfed Baby
- Continues to lose weight after day-5
- Below birth weight at day-14
- Gaining less than 120g per week after the first week, or less than 500g per month.
- Less than six wet nappies daily
- Urine that is yellow and strong smelling
- Infrequent dry, hard, green stools
- Worried-looking face
- Not alert, active and reasonably content for some periods daily
- Unusually lethargic and sleepy
- Weak cry
- Obviously unhappy, restless, fussy and dissatisfied after breastfeeding.
Signs of Breasts Over-Producing Milk
- Baby gets uncomfortable, cries incessantly, is windy and has frequent green stools (maybe with mucus).
- When feeding on one side, other breast leaks a lot of milk (beyond the first few weeks).
- When baby pulls off the nipple, milk squirts some distance.
- During feeding, mother hears a 'milk hitting the bottom of the tummy' sound.
- Baby seemingly in pain, for feeding stimulates bowel movements.
- Baby 'head-bangs' during feeds, arching its back, and pulling off the breast to protect its airway, perhaps dragging the nipple with it, then maybe refusing to feed.
- NOTE: With the fast rush of milk, the baby can swallow a lot of air as well as milk, which can make the baby think they're full.
Feeding options and requirements
Exclusive breastfeeding means feeding a baby nothing but breast milk. Predominant or mixed breastfeeding means feeding breast milk along with some form of substitute – infant formula or baby food and even water, depending upon the age of the child. Babies feed differently with artificial teats than from a breast. When feeding from the breast, the tongue massages the milk out rather than sucking, and the nipple does not go as far into the mouth; when feeding from a bottle, an infant will suck harder. Therefore the advice is not to mix breastfeeding and bottle-feeding (or the use of a pacifier) until the baby is used to feeding from its mother. Orthodontic teats, which are generally slightly longer, can be used to better replicate the breast.
Exclusively breastfed infants feed, on average, 6-14 times a day. The requirement varies greatly among children. Newborns consume about 30 to 90 ml (1 to 3 US fluid ounces), and after the age of four weeks, babies consume about 120ml (4 US fluid ounces) per feed. Each baby is different, and as it grows the amount will increase. It is important to recognise the signs of a baby's hunger and it is advised that the baby should dictate the number, frequency, and length of each feed, based on the assumption that it knows how much milk it needs. The supply of milk in the breast is determined by the frequency and length of these feeds or the amount of milk expressed. The birth weight of the baby may affect its feeding habits, and mothers may be influenced by what they perceive its requirements to be. For example, a baby born small for gestational age may lead a mother to believe that her child needs to feed more than if it larger; they should, however, go by the demands of the baby rather than what they feel is necessary.
One limitation of breastfeeding is that it is harder to accurately measure the amount of food the baby consumes. Since a baby will normally feed to meet its own requirements, this is rarely a problem except when attempting to determine a cause for undernutrition. It is possible to guess output from wet and soiled nappies: 8 wet cloth or 5-6 wet disposable, and 2-5 soiled per 24 hours) suggests an acceptable amount of input for newborns older than 5-6 days old. After 2-3 months, stool frequency is a less accurate measure of adequate input as some normal infants may go up to 10 days between stools.
Expression

{kind=link}
Manual breast pump
When direct breastfeeding is not possible a baby may still be fed breast milk. By expressing (artificially removing and storing) her milk, a mother can enable her child to be fed while she is away from the child. With expression through manual massage or the use of a breast pump the woman can draw out her milk and keep it in supplemental nursing system or a bottle ready for use. This bottle may be kept on the counter for up to seven hours, refrigerated for up to eight days or frozen for up to four months. Research suggests that antioxidant activity in expressed breast milk decreases over time [11] but it still remains in higher levels than in infant formula.
Expression can be used to maintain lactation, such as when the mother and child are separated for an extended period. If the baby is unable to feed, expressed milk can be fed through a nasogastric tube.
Expressed milk can also be used to help a mother who is having difficulty breastfeeding, such as when a newborn causes grazing and bruising or when an older baby grows teeth and bites the nipple (though the reaction of the mother to a bite - a jump and a cry of pain - is usually enough to discourage the child from biting again).
Some women donate their expressed breast milk (EBM) to others, either directly or through the hospital. Though some dislike the idea of feeding their own child with another person's milk, others appreciate the ability to give their baby the benefits of breast milk. Feeding an infant breast milk is more important in some situations than in others, such as for a premature baby.
Infant formula


{kind=link}
Expressed breast milk (EBM) or infant formula can be fed to an infant by bottle
The World Health Organization recommends that all mothers be encouraged to breastfeed.[1] Hospitals that are accredited by the World Health Organization are tolerant of formula feeding but do not offer it to infants who can be breastfed. (Feeding a new baby with formula undermines the establishment of breastfeeding.)
If the decision is made not to feed the child breast milk, or if breastfeeding is not possible, then infant formula can be given to the infant, usually using a baby bottle. Infant formula may also be introduced as a supplemental liquid drink to weaned babies. Because it is proportioned for human babies it may be seen as healthier than simply drinking the milk from another mammal.
While it is inferior to breastfeeding, infant formula has been effectively marketed and promoted to new mothers as a modern, easy or convenient option to feeding a baby. A 2004 UK Department of Health survey showed that 34% of women believe infant formula to be very similar to or the same as breast milk. [12] In 1979 the International Baby Food Action Network (IBFAN) was formed to help raise awareness of such practices as supplementary feeding of new babies with formula, inappropriate promotion of baby formula and to help change attitudes that discourage or inhibit mothers from breastfeeding their babies.
Feeding two infants simultaneously is called tandem breastfeeding. The most common need for this is after the birth of twins whereby both babies are fed at the same time. It is not necessarily the case, however, that the appetite and feeding habits of both babies are the same. This leads to the complication of trying to feed each baby according to its own individual requirements while also trying to breastfeed them both at the same time.
In cases of multiple births with three or more children it is extremely difficult for the mother to organise feeding around the appetites of all of the babies. The breasts can produce a high quantity of milk, according to the demand placed upon them, and many mothers have been able to feed their infants successfully [13]. It is common, however, for the woman to use other alternatives.
Tandem breastfeeding is also convenient if a woman gives birth to a newborn while still feeding an older baby or child. Under these circumstances during the late stages of pregnancy the milk will change to colostrum for the benefit of the newborn. Some older nurslings will continue to feed even with this change while others may wean due to the change in taste.
Although some may find it controversial, some women breastfeed their offspring for as many as 3 to (rarely) 7 years from birth. This is referred to as extended breastfeeding. Supporters of extended breastfeeding say that all the benefits of human milk, both nutritional and emotional, continue for as long as a child nurses. Detractors believe that prolonging breastfeeding for several years can result in the child developing emotional or psycho-sexual problems, though there is no research that supports this theory. There has, however, been at least one study linking extended breastfeeding with adverse cardiac outcomes later in life.[14]
In developing nations within Africa and elsewhere, it is sometimes common for more than one woman to feed a child. This shared breastfeeding has been highlighted as a source of HIV infection amongst infants born HIV-negative [15].
See also: wet nurse
Breastfeeding method
There are many texts available to new mothers to assist in the establishment of breastfeeding. The baby will usually indicate hunger by crying or moaning and fussing. When the baby's cheek is stroked, the baby will move his or her face towards the stroking and open his or her mouth, demonstrating the rooting instinct. Breastfeeding can make the mother thirsty and can last for up to an hour (usually in the early days, when both mother and baby are inexperienced) – it is therefore common for the mother to replace lost water by drinking during the process.
Feeding and positioning
{kind=link}
It is essential for the infant to feed in the correct position and with an adequate latch.
While for some people the process of breastfeeding seems natural there is a level of skill required for successful feeding and a correct technique to use. Incorrect positioning is one of the main reasons for unsuccessful feeding and can easily cause pain in the nipple or breast. By stroking the baby's cheek with the nipple the baby will open its mouth and turn toward the nipple, which should then be pushed in so that the baby has a mouthful of nipple and areola; the nipple should be at the back of the baby's throat. Achievement of this position is referred to as latching on. Inverted or flat nipples can be massaged to give extra area for the baby to latch onto. Many women choose to wear a nursing bra to allow easier access to the breast than normal bras.
The baby may pull away from the nipple after a few minutes or after a much longer period of time. Sometimes the baby will re-latch on the same breast or mother may offer the other side. The fat content of the milk increases as the breast empties.
The length of feeding is quite variable. Regardless of the duration, it is important for the breastfeeding woman to be comfortable.
- Upright: The sitting position with the back straight.
- Mobile: The mother carries her nursling in a sling or other baby carrier while breastfeeding. Doing so permits the mother to incorporate breastfeeding into the varied work of daily life.
- Lying down: Good for night feeds or for those who have had a caesarean section.
- On her back: Mother is usually sitting slightly upright; particularly useful for tandem breastfeeding.
- On her side: The mother and baby lie on their sides.
- Hands and knees: The mother is on all fours with the baby underneath her (not usually recommended).
There are many positions and ways in which the feeding infant can be held. This depends upon the comfort of the mother and child and the feeding preference of the baby – some babies tend to prefer one breast to another. Most women breastfeed their child in the cradling position.
- Cradling positions:
- Football hold: The woman is upright and the baby is held securely under the mother's arm with the head cradled in her hands.[17]
- Feeding up hill: The baby lies stomach to stomach with the mother who is lying on her back; this is helpful for babies finding it difficult to feed.
- Lying down:
- On its side: The mother and baby lie on their sides.
- On its back: The baby is lying on its back (cushioned by something soft) with the mother on her hands and knees above the child (not usually recommended).
When tandem breastfeeding the mother is unable to move the baby from one breast to another and comfort can be more of an issue. This brings extra strain to the arms, especially as the babies grow, and many mothers of twins recommend the use of more supporting pillows. Favoured positions include:
- Double cradle hold
- Double clutch hold[18]
- One clutched baby and one cradled baby
- Lying down
Breast and nipple pain
Breastfeeding may hurt some women. Sometimes this is related to an incorrect technique, but it usually eases over time. Milk ducts can block up on occasion, leading to breast engorgement or mastitis, and should be addressed with massage and by encouraging the baby to suck from that side to keep it as empty as possible until the problem goes away. The presence of thrush in the nipples can also be painful. Limiting feeding time does not prevent soreness.
Although it is said that fair skinned mothers are most likely to experience cracked nipples, cracked nipples can happen to anyone whose baby is not positioned correctly. The baby's rough tongue can also cause grazes and the suction can cause bruising if the mother and baby have not learned to latch and unlatch. To break the suction, mothers should wait for the baby to come off the breast, insert a finger just inside the baby's mouth, or press down gently on the breast. The use of nursing pads or tight bras can lead to breast and nipple pain, as can hair dryers, sun lamps, soap, alcohol, perfume, deodorant, hair spray, body powder and incorrect use of breast pumps. Bottles and nipple shields may change the way the baby sucks, as well.
Some mothers apply medical grade lanolin to sooth nipples; La Leche League International has endorsed Lansinoh, an ultra pure medical grade lanolin cream designed for breastfeeding mothers. Mothers can also express milk and rub it on the nipples.[19] After six weeks of breastfeeding, the process usually becomes easier, as both mother and baby learn the best technique. Mothers can also buy or rent breast pumps to extract the milk, if nipple pain becomes unbearable. It should be noted, however, that pumping breast milk can also be associated with nipple pain, and is best used only as a temporary solution while the most common culprit, a poor latch, is improved.
Nipple damage due to breastfeeding can increase the likelihood of a Candidiasis infection. If a baby develops symptoms of oral thrush, both the mother and the child must be treated at the same time.[20] Proper antifungal treatment will help neutralise the infection and aid in the nipple healing process.
Weaning
Weaning is the process of gradually introducing the infant to what will be its adult diet and withdrawing the supply of milk. The infant is considered to be fully weaned once it no longer receives any breast milk and begins to rely on baby food or other solid foods for all its nutrition. Most mammals cease the production of the enzyme lactase at the end of weaning, becoming lactose intolerant. Many humans have a mutation that allows the production of lactase throughout life and can drink milk well beyond the age of weaning [21]. Typically, this milk comes from domesticated animals.
History of breastfeeding


{kind=link}
An early 20th century Korean woman wearing a traditional breastfeeding clothing.


{kind=link}
Two early 20th century Korean women feeding their babies while working.
In the early years of the human species, breastfeeding was as common as it was for other mammals feeding their young. There were no alternative foods for the infants, and the mother, along with other lactating females, would have no choice but to breastfeed the children. This process is still seen in many developing countries and is known as shared breastfeeding.
The Egyptian, Greek and Roman empires saw women only feeding their own children. However, breastfeeding began to be seen as something too common to be done by royalty, and wet nurses were employed to breastfeed the children of the royal families. This was extended over the ages, particularly in western Europe, and saw women of noble birth (or who married into nobility) making use of wet nurses.
According to some Brahminical literature, breastfeeding in 2nd century India was commonly practised but not until the fifth day, allowing the colostrum to be discarded and the true breast milk to flow.
Developing alternatives
Alternatives first became popular in the late 15th century with many parents substituting cow or goat's milk for their own breast milk. This was particularly necessary for those families working the land whereby time could not easily be taken out to regularly breastfeed the child. Such trends soon faded when the problems associated with these milks started to show, and by the mid to late 16th century breastfeeding once again became the preferred feeding method for most families.[citation needed] The Italian Hieronymus Mercurialis wrote in 1583 that women generally finished breastfeeding an infant exclusively after the third month and entirely after around 13 months.
Dry nursing, the feeding of flour or cereal mixed with broth or water, became the next alternative in the 19th century but once again quickly faded. Around this time there became an obvious disparity in the feeding habits of those living in rural areas and those in urban areas. Most likely due to the availability of alternative foods, babies in urban areas were breastfed for a much shorter length of time, supplementing the feeds earlier than those in rural areas.
Though first developed by Henri Nestlé in the 1860s, infant formula received a huge boost during the post World War II "Baby Boom". The aggressive marketing campaigns when business and births decreased saw Nestlé and other such companies focus on non-industrialised countries, while government strategies in industrialised countries attempted to highlight the benefits of breastfeeding.
Breastfeeding in Japan
Traditionally, Japanese babies were born at home and breastfed with the help of breast massage. Weaning was often late, with breastfeeding in rare cases continuing until early adolescence. After World War II Western medicine was taken to Japan and the women began giving birth in hospitals, where the baby was usually taken to the nursery and fed formula. In 1974 a new breastfeeding promotion by the government helped to boost the awareness of its benefits and the uptake has seen a sharp increase. Japan became the first developed country to have a Baby-friendly hospital (and has since gone on to have another 24 such facilities).
Breastfeeding in Canada
A 1994 Canadian government health survey found that 73% of Canadian mothers initiated breastfeeding, up from 38% in 1963. It has been speculated that the gap between breastfeeding generations in Canada contributes to lack of success of those who do attempt it: new parents cannot look to older family members for help with breastfeeding since they are also ignorant on the topic. [22] Western Canadians are more likely to breastfeed; just 53% of Atlantic province mothers breastfeed, compared to 87% in British Columbia. More than 90% of women surveyed said they breastfeed because it provides more benefits for the baby than does formula. Of women who did not breastfeed, 40% said formula feeding was easier (the most prevalent answer). Women who were older, more educated, had higher income, and were married were the most likely to breastfeed. Immigrant women were also more likely to breastfeed. About 40% of mothers who breastfeed do so for less than three months. Women were most likely to discontinue breastfeeding if they perceived themselves to have insufficient milk. However, among women who breastfed for more than three months, returning to work or a previous decision to stop at that time were the top reasons.
A 2003 La Leche League International study found that 72% of Canadian mothers initiate breastfeeding and that 31% continue to do so past four to five months.[23]
A 1996 article in the Canadian Journal of Public Health found that, in Vancouver, 82.9% of mothers initiated breastfeeding, but that this differed by Caucasian (91.6%) and non-Caucasian (56.8%) women.[24] The article reported that just 18.2% of mothers breastfeed at nine months, and that breastfeeding practices were significantly associated with the mothers' marital status, education and family income.
Typically, if a baby is born in a hospital in Canada, the mother will be given a bottle filled with formula "just in case" she has any problems breastfeeding. However, faced with unfamiliar emotions just after giving birth, with hormones suddenly dropping, and with no help from hospital staff, breastfeeding frustration is not uncommon, and the bottle becomes a source of welcome relief rather than a last resort.
Breastfeeding in Cuba
Since 1940, Cuba's constitution has contained a provision officially recognising and supporting breastfeeding. Article 68 of the 1975 constitution reads, in part: During the six weeks immediately preceding childbirth and the six weeks following, a woman shall enjoy obligatory vacation from work on pay at the same rate, retaining her employment and all the rights pertaining to such employment and to her labour contract. During the nursing period, two extraordinary daily rest periods of a half hour each shall be allowed her to feed her child.
Publicity, promotion and law
{kind=link}
Lucy Lawless (actress for Xena: Warrior Princess) promotional poster for World Breastfeeding Week.
In response to public pressure, the health departments of various governments have recognised the importance of encouraging women to breastfeed. The required provision of baby changing facilities was a large step towards making places more accessible for parents and in many countries there are now laws in place to protect the rights of a breastfeeding mother when feeding her child in public.
The World Health Organization (WHO), along with grassroots non-governmental organisations like the International Baby Food Action Network (IBFAN) have played a large role in encouraging these governmental departments to promote breastfeeding. Under this advice they have developed national breastfeeding strategies, including the promotion of its benefits and attempts to encourage mothers, particularly those under the age of 25, to choose to feed their child with breast milk.
Government campaigns and strategies around the world include:
- National Breastfeeding Week in the UK
- The Department of Health and Ageing Breastfeeding Strategy in Australia
- The National Women's Health Information Center in the U.S.
- La Leche League International, a volunteer mother-to-mother international group.
- World Breastfeeding Week
However, there has been a long, ongoing struggle between corporations promoting artificial substitutes and grassroots organisations and WHO defending breastfeeding. The International Code of Marketing of Breast-milk Substitutes was developed in 1981 by WHO, but violations have been reported by organisations, including those networked in IBFAN. In particular, Nestlé took three years before it initially implemented the code, and in the late 1990s and early 2000s was again found in violation. Nestlé had previously faced a boycott, beginning in the US but soon spreading through the rest of the world, for marketing practices in the third world (see Nestlé boycott).
Developing nations
In many countries, particularly those with a generally poor level of health, malnutrition is the majority cause of death in children under 5, with 60% of all those cases being within the first year of life [25]. International organisations such as Plan International and La Leche League have helped to promote breastfeeding around the world, educating new mothers and helping the governments to develop strategies to increase the number of women exclusively breastfeeding.
Traditional beliefs in many developing countries give different advice to women raising their newborn child. In Ghana babies are still frequently fed with tea alongside breastfeeding [26]. This reduces the benefits of exclusive breastfeeding and the drink can inhibit the absorption of iron, important in the prevention of anaemia.
Breastfeeding in public
When in public with a breastfed baby it is often difficult to avoid the need to feed the infant. Therefore legal and social rules regarding indecent exposure and dress code, as well as inhibitions of the woman, tend to be relaxed for this situation. There are numerous laws around the world that have made public breastfeeding legal and disallow companies from prohibiting it in the workplace. Yet, the public reaction at the sight of breastfeeding can make the situation uncomfortable for those involved.
In the U.S. an appropriations bill (H.R.2490) with a breastfeeding amendment (H.AMDT.295 to H.R.2490) was signed into law on September 29, 1999 affirming the right of a woman to breastfeed her child anywhere on federal property. However, not all state laws have affirmed the same right in their respective public places. Recent attempts to codify a child's right to nurse found success in Ohio, but failed in West Virginia and some other states. By June 2005, 35 states had enacted legislation to protect breastfeeding mothers and their children. Laws protecting the right to nurse aim to change attitudes and promote increased incidence and duration of breastfeeding. Nowhere is breastfeeding in public illegal.
A survey reported by the UK Department of Health stated that most people (84%) find breastfeeding in public acceptable as long as it is done discreetly [27]. Contrastingly, 67% of mothers are worried about general opinion being against public breastfeeding. To combat these fears in Scotland, a bill [28] (pdf) safeguarding the freedom of women to breastfeed in public has been passed [29] in the Scottish Parliament [30]. The legislation sets up a fine of up to £2500 for preventing breastfeeding in legally permitted places.
In Canada, the Canadian Charter of Rights and Freedoms affords some protection under sex equality. Although Canadian human rights protection does not explicitly include breastfeeding, a 1989 Supreme Court of Canada decision (Brooks v. Canadian Safeway Ltd.) set the precedent for pregnancy as a condition unique to women and that thus discrimination on the basis of pregnancy is a form of sex discrimination. Canadian legal precedent also allows women the right to bare their breasts, just as men may. In British Columbia, the British Columbia Human Rights Commission Policy and Procedures Manual protects the rights of female workers who wish to breastfeed.
Some mothers choose to pump or express milk by hand so that they can carry a small bottle of milk with them if they plan to be out at mealtimes.
Recent global uptake
The following table shows the uptake of exclusive breastfeeding. Sources: WHO Global Data Bank on Breastfeeding and UNICEF Global Database Breastfeeding Indicators
| Country | Percentage | Year | Type of feeding |
|---|---|---|---|
| Armenia | 0.7% | 1993 | Exclusive |
| 20.8% | 1997 | Exclusive | |
| Benin | 13% | 1996 | Exclusive |
| 16% | 1997 | Exclusive | |
| Bolivia | 59% | 1989 | Exclusive |
| 53% | 1994 | Exclusive | |
| Central African Republic | 4% | 1995 | Exclusive |
| Chile | 97% | 1993 | Predominant |
| Colombia | 19% | 1993 | Exclusive |
| 95% (16%) | 1995 | Predominant (exclusive) | |
| Dominican Republic | 14% | 1986 | Exclusive |
| 10% | 1991 | Exclusive | |
| Ecuador | 96% | 1994 | Predominant |
| Egypt | 68% | 1995 | Exclusive |
| Ethiopia | 78% | 2000 | Exclusive |
| Mali | 8% | 1987 | Exclusive |
| 12% | 1996 | Exclusive | |
| Mexico | 37.5% | 1987 | Exclusive |
| Niger | 4% | 1992 | Exclusive |
| Nigeria | 2% | 1992 | Exclusive |
| Pakistan | 12% | 1988 | Exclusive |
| 25% | 1992 | Exclusive | |
| Poland | 1.5% | 1988 | Exclusive |
| 17% | 1995 | Exclusive | |
| Saudi Arabia | 55% | 1991 | Exclusive |
| Senegal | 7% | 1993 | Exclusive |
| South Africa | 10.4% | 1998 | Exclusive |
| Sweden | 55% | 1992 | Exclusive |
| 98% | 1990 | Predominant | |
| 61% | 1993 | Exclusive | |
| Thailand | 90% | 1987 | Predominant |
| 99% (0.2%) | 1993 | Predominant (exclusive) | |
| 4% | 1996 | Exclusive | |
| United Kingdom [31] | 62% | 1990 | |
| 66% | 1995 | ||
| Zambia | 13% | 1992 | Exclusive |
| 23% | 1996 | Exclusive | |
| Zimbabwe | 12% | 1988 | Exclusive |
| 17% | 1994 | Exclusive | |
| 38.9% | 1999 | Exclusive |
Lactation without pregnancy
Although it is not widely known in developed countries, women who have never been pregnant are sometimes able to stimulate lactation sufficient to breastfeed. This is called "induced lactation", while a woman who has lactated before and re-starts is said to "relactate". If the nipples are stimulated as in breastfeeding for a while (such as by a breast pump or actual suckling), eventually the breasts will begin to produce milk which can be used to feed a baby. Once established, lactation adjusts to demand. For this reason, adoptive mothers, usually initially in conjunction with some form of supplementation, such as a supplemental nursing system, are able to breastfeed their infants and young children [32]. There is thought to be little or no difference in milk composition whether lactation is induced or a result of pregnancy. Rare accounts of male lactation (as distinct from galactorrhea) exist in the medical literature.
Some couples may choose to induce lactation as a solely sexual practice.
Additionally, some drugs, primarily atypical antipsychotics such as Risperdal, may cause lactation in both women and men.
See also
- Attachment parenting
- Baby-friendly hospital
- Continuum concept
- Lactation
- List of child related articles
- Milk fetishism
- Parenting
- Roman Charity
- Topfree equality
- Breast milk
- Breast pump
References
Numbered references
- ↑ 1.0 1.1 Exclusive Breastfeeding. WHO: Child and Adolescent Health and Development. URL accessed on 2006-05-03.
- ↑ Gartner LM, Morton J, Lawrence RA, Naylor AJ, O'Hare D, Schanler RJ, Eidelman AI (2005). Breastfeeding and the use of human milk. Pediatrics 115 (2): 496-506. PMID 15687461 fulltext.
- ↑ 3.0 3.1 3.2 Nancy Mohrbacher, Julie Stock, LA Leche League International (2003). The Breastfeeding Answer Book, 3rd ed. (revised), La Leche League International. ISBN 0-912500-92-1.
- ↑ 4.0 4.1 4.2 Rilemma 1994
- ↑ Cregan 2002
- ↑ Sears, MD, William; Sears, RN, Martha: The Breastfeeding Book, Little, Brown, 2002. ISBN 0316779245
- ↑ Hopkinson 1988
- ↑ deCarvalho 1985
- ↑ Daly 1993
- ↑ AAP, 1997
- ↑ 11.0 11.1 11.2 Fray, K: "Oh Baby...Birth, Babies & Motherhood Uncensored, pages 173-184, Random House NZ, 2005. ISBN 1-86941-713-5
Unnumbered references
- Breastfeeding, Biocultural Perspectives; Editors Patricia Stuart-Macadam & Katherine A. Dettwyler.
- Hausman, Bernice (2003). Mother's Milk: Breastfeeding Controversies in American Culture. New York: Routledge. ISBN 0-41596-656-6
- Huggins, Kathleen (1999). The Nursing Mother's Companion. Harvard Common Press; 4th edition. ISBN 1-55832-152-7
- Lothrop, H. (1998). Breastfeeding Naturally, Fisher Books, USA. ISBN 1-55561-131-1
- Mercurialis, H. (1583). De Morbis Puerorum.
- Minchin, M. (1985). Breastfeeding matters, Almo Press Publications, Australia. ISBN 0-86861-810-1
- Moody, J., Britten, J. and Hogg, K. (1996). Breastfeeding your baby, National Childbirth Trust, UK. ISBN 0-72253-635-6
- Pryor, Gail. (1996). Nursing Mother, Working Mother: The Essential Guide for Breastfeeding and Staying Close to Your Baby After You Return to Work. Harvard Common Press ISBN 1-55832-117-9.
- Royal College of Midwives (1991). Successful Breastfeeding: A Practical Guide for Midwives, Royal College of Midwives, London.
- Stuart-Macadam, P. and Dettwyler, K. (1995). Breastfeeding: Biocultural Perspectives (Foundations of Human Behavior), Aldine de Gruyter. ISBN 0-20201-192-5
- Perez-Reyes M, Wall ME Presence of delta9-tetrahydrocannabinol in human milk. N Engl J Med 1982; 307:819-820 PMID 6287261
- Astley SJ, Little RE., Maternal marijuana use during lactation and infant development at one year. Neurotoxicol Teratol. 1990 Mar-Apr;12(2):161-8. PMID 2333069
- Leeson CPM, Kattenhorn M, Deanfield JE, Lucas A Duration of breast feeding and arterial distensibility in early adult life: population based study BMJ, Mar 2001; 322: 643 - 647.
Other Well Known Authors on Breastfeeding
- Arlene Eisenberg
- Hale Thomas (Medications in Mothers Milk)
- Sheila Kitzinger
- La Leche League International
- Francesca Naish & Janette Roberts
- Miriam Stoppard
Website references
- American Academy of Pediatrics Policy Statement on Breastfeeding
- 4woman.gov – US Department of Health & Human Services Breastfeeding resource page
- Breastfeeding NHS – UK NHS Breastfeeding strategy
- Royal Australasian College of Physicians Paediatric Policy: Brreastfeeding
- ADC Online journals
- American Family Physician Initial Management of Breastfeeding by Keith Sinusas and Amy Galgliardi
- Linkages Project Benefits of Breastfeeding USAID Program
- Benefits of breastfeeding United States Breastfeeding Committee
- Breastfeeding is Priceless No Substitute for Human Milk Coalition for Improving Maternity Services
- Breastfeed-essentials.com
- Plan International
- La Leche League International – An international organisation whose mission is to help mothers worldwide to breastfeed through mother-to-mother support, encouragement, information, and education and to promote a better understanding of breastfeeding as an important element in the healthy development of the baby and mother
- WhyQuit.com – Anti-smoking site with numerous links in the "Known Breastfeeding Risk Factors" section
- Mama's Baby: Happy, Healthy and Breastfed Black Women's health Imperative
- The Adoptive Breastfeeding Resource Website
Infant pain and breastfeeding
- American Academy of Pediatrics. Committee on Psychosocial Aspects of Child and Family Health; Task Force on Pain in Infants, Children, and Adolescents. The assessment and management of acute pain in infants, children, and adolescents. Pediatrics. 2001 Sep;108(3):793-7.
- Howard CR, Howard FM, Weitzman ML. Acetaminophen analgesia in neonatal circumcision: the effect on pain. Pediatrics. 1994;93(4):641-6.
- The Womanly Art of Breastfeeding, Third Edition, July 1981. Pages 92-93 Elective Surgery for you or baby
- See also the section on circumcision and breastfeeding in Medical analysis of circumcision
Health risks of formula feeding
- Health risks of not breastfeeding US Department of Health & Human Services
- The Risks of Infant Formula Feeding breastfeeding task force of greater Los Angeles
- Breastfeeding and the Risk of Postneonatal Death in the United States Pediatrics, Vol. 113 No. 5 May 2004 & resulting correspondence
- Supplementation of the Breastfed Baby "Just One Bottle Won't Hurt" ...or Will It? by Marsha Walker RN IBCLC (National Alliance for Breastfeeding Advocacy)
- Salon.com Formula for disaster by Katie Allison Granju
- What should I know about infant formula? Kellymom.com (contains links to other websites)
- National Alliance for Breastfeeding Advocacy contains links to other articles including:
- Contaminents in Infant Formula
- Recalls of Infant Feeding Products
- Antidepressants, Antipsychotics, Benzodiazepines, and the Breastfeeding Dyad Perspectives in Psychiatric Care, Apr-Jun 2004, by Kirsten J. Malone This article discusses the risks to both mother and child of formula feeding and attempts to weigh them against the risk to infants of absorbing psychotropic druge through breastmilk.
External links
- Australian Breastfeeding Association — Informative website and forum
- Baby Milk Action — Supports mothers' rights to breastfeed
- Breastfeeding information & resources from Seattle Children's Hospital
- Canadian Breastfeeding Rights — from Canadian Infant Feeding Action Coalition
- Comparison of Human Milk and Formula
- Human Milk Secretion: An Overview
- Kellymom.com — Providing evidence based breastfeeding information
- Read Congressional Research Service (CRS) Reports regarding Breastfeeding and U.S. law
- U.S. Food and Drug Administration (FDA) "Breast-Feeding Best Bet for Babies"
- WHO — Infant and Young Child Feeding Practices
Videos
da:Amme de:Stillen es:Amamantar fi:Imetys fi:Rintaruokinta fr:Allaitement he:הנקה lt:Žindymas nl:Borstvoeding no:Amming pt:Aleitamento ru:Грудное вскармливание sv:Amning zh:母乳喂养
| This page uses Creative Commons Licensed content from Wikipedia (view authors). |