Assessment |
Biopsychology |
Comparative |
Cognitive |
Developmental |
Language |
Individual differences |
Personality |
Philosophy |
Social |
Methods |
Statistics |
Clinical |
Educational |
Industrial |
Professional items |
World psychology |
Biological: Behavioural genetics · Evolutionary psychology · Neuroanatomy · Neurochemistry · Neuroendocrinology · Neuroscience · Psychoneuroimmunology · Physiological Psychology · Psychopharmacology (Index, Outline)
{kind=link}
Lovastatin, a compound isolated from Aspergillus terreus, was the first statin to be marketed for lowering cholesterol.
{kind=link}
The "oyster mushroom", a culinary mushroom, naturally contains up to 2.8% Lovastatin on a dry weight basis.[1]
The statins (or HMG-CoA reductase inhibitors) are a class of drugs that lower cholesterol levels in people.
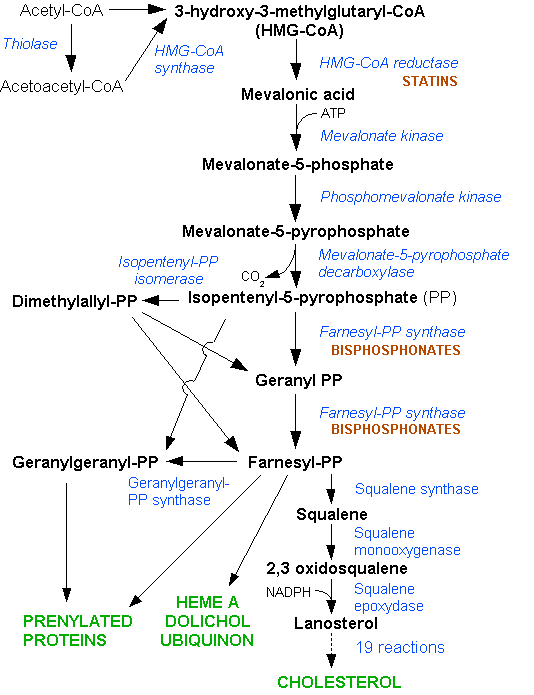
They lower cholesterol by inhibiting the enzyme HMG-CoA reductase, which is the rate-limiting enzyme of the mevalonate pathway of cholesterol synthesis. Inhibition of this enzyme in the liver results in decreased cholesterol synthesis as well as increased synthesis of LDL receptors, resulting in an increased clearance of low-density lipoprotein (LDL) from the bloodstream. The first results can be seen after one week of use and the effect is maximal after four to six weeks.
History
Akira Endo and Masao Kuroda of Tokyo, Japan commenced research into inhibitors of HMG-CoA reductase in 1971 (Endo 1992). This team reasoned that certain microorganisms may produce inhibitors of the enzyme to defend themselves against other organisms, as mevalonate is a precursor of many substances required by organisms for the maintenance of their cell wall (ergosterol) or cytoskeleton (isoprenoids).[2]
The first agent isolated was mevastatin (ML-236B), a molecule produced by the fungus Penicillium citrinum. The pharmaceutical company Merck & Co. showed an interest in the Japanese research in 1976, and isolated lovastatin (mevinolin, MK803), the first commercially marketed statin, from the fungus Aspergillus terreus. Dr. Endo was awarded the 2006 Japan Prize for his work on the development of statins, and the Clinical Medical Research Award from the Lasker Foundation in 2008.
Mechanism of action
{kind=link}
The HMG-CoA reductase pathway, which is blocked by statins via inhibiting the rate limiting enzyme HMG-CoA reductase.
- Main article: Cholesterol#Homeostasis
Statins act by competitively inhibiting HMG-CoA reductase, the first committed enzyme of the HMG-CoA reductase pathway. Because statins are similar to HMG-CoA on a molecular level they take the place of HMG-CoA in the enzyme and reduce the rate by which it is able to produce mevalonate, the next molecule in the cascade that eventually produces cholesterol, as well as a number of other compounds. This ultimately reduces cholesterol via several mechanisms.
Inhibiting cholesterol synthesis
By inhibiting HMG-CoA reductase, statins block the pathway for synthesizing cholesterol in the liver. This is significant because most circulating cholesterol comes from internal manufacture rather than the diet. When the liver can no longer produce cholesterol, levels of cholesterol in the blood will fall. Cholesterol synthesis appears to occur mostly at night,[3] so statins with short half-lives are usually taken at night to maximize their effect. Studies have shown greater LDL and total cholesterol reductions in the short-acting simvastatin taken at night rather than the morning,[4][5] but have shown no difference in the long-acting atorvastatin.[6]
Increasing LDL uptake
Liver cells sense the reduced levels of liver cholesterol and seek to compensate by synthesizing LDL receptors to draw cholesterol out of the circulation.[7] This is accomplished via protease enzymes that cleave a protein called "membrane-bound sterol regulatory element binding protein", which migrates to the nucleus and causes increased production of various other proteins and enzymes, including the LDL receptor. The LDL receptor then relocates to the liver cell membrane and binds to passing LDL and VLDL particles (the "bad cholesterol" linked to disease). LDL and VLDL are drawn out of circulation into the liver and are digested.
Other effects
Statins exhibit action beyond lipid-lowering activity in the prevention of atherosclerosis. The [[ASTEROnuary 1999|pages=185–188|pmid=9892578 |issue=2 }}</ref>
- Improve endothelial function
- Modulate inflammatory responses
- Maintain plaque stability
- Prevent thrombus formation
Statins may even benefit those without high cholesterol. In 2008 the JUPITER study showed fewer stroke, heart attacks, and surgeries even for patients who had no history of high cholesterol or heart disease, but only elevated C-reactive protein levels. There were also 20% fewer deaths (mainly from reduction in cancer deaths) though deaths from cardiovascular causes were not reduced.[8]
Statins have been linked to a marked reduction in prostate cancer, benign prostate enlargement, incontinence and impotence in older men.[9]
Indications and uses
Statins, the most potent cholesterol-lowering agents available, lower LDL cholesterol (so-called "bad cholesterol") by 1.8 mmol/l. This translates in a 60% decrease in the number of cardiac events (heart attack, sudden cardiac death), and a 17% reduced risk of stroke.[10] They have less effect than the fibrates or niacin in reducing triglycerides and raising HDL-cholesterol ("good cholesterol"). Professional guidelines generally require that the patient has tried a cholesterol-lowering diet before statin use is considered; statins or other pharmacologic agents may then be recommended for patients who do not meet their lipid-lowering goals through diet and lifestyle approaches.
The indications for the prescription of statins have broadened over the years. Initial studies, such as the Scandinavian Simvastatin Survival Study (4S), supported the use of statins in secondary prevention for cardiovascular disease, or as primary prevention only when the risk for cardiovascular disease was significantly raised (as indicated by the Framingham risk score).[11] Indications were broadened considerably by studies such as the Heart Protection Study (HPS), which showed preventative effects of statin use in specific risk groups, such as diabetics. The ASTEROID trial, published in 2006, using only a statin at high dose, achieved lower than usual target calculated LDL values and showed disease regression within the coronary arteries using intravascular ultrasonography.[12]
Based on clinical trials, the National Cholesterol Education Program guidelines, and the increasing focus on aggressively lowering LDL-cholesterol, the statins continue to play an important role in both the primary and secondary prevention of coronary heart disease, myocardial infarction, stroke and peripheral artery disease.
Research continues into other areas where statins also appear to have a favorable effect: colon cancer [13] ,inflammation, dementia,[14] lung cancer,[15] nuclear cataracts,[16] and hypertension.[17]
Members
Fermentation-derived and synthetic
The statins are divided into two groups: fermentation-derived and synthetic.
The statins include, in alphabetical order (brand names vary in different countries):
| Statin | Image | Brand name | Derivation |
| Atorvastatin | Lipitor, Torvast | Synthetic | |
| Cerivastatin | Lipobay, Baycol. (Withdrawn from the market in August, 2001 due to risk of serious Rhabdomyolysis) | Synthetic | |
| Fluvastatin | Lescol, Lescol XL | Synthetic | |
| Lovastatin | Mevacor, Altocor, Altoprev | Fermentation-derived. Naturally-occurring compound. Found in oyster mushrooms and red yeast rice. | |
| Mevastatin | - | Naturally-occurring compound. Found in red yeast rice. | |
| Pitavastatin | Livalo, Pitava | Synthetic | |
| Pravastatin | Pravachol, Selektine, Lipostat | Fermentation-derived | |
| Rosuvastatin | Crestor | Synthetic | |
| Simvastatin | Zocor, Lipex | Fermentation-derived. (Simvastatin is a synthetic derivate of a fermentation product) | |
| Simvastatin+Ezetimibe | Vytorin | Combination therapy | |
| Lovastatin+Niacin extended-release | Advicor | Combination therapy | |
| Atorvastatin+Amlodipine Besylate | Caduet | Combination therapy - Cholesterol+Blood Pressure | |
| Simvastatin+Niacin extended-release | Simcor | Combination therapy |
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
LDL-lowering potency varies between agents. Cerivastatin is the most potent, followed by (in order of decreasing potency), rosuvastatin, atorvastatin, simvastatin, lovastatin, pravastatin, and fluvastatin.[18] The relative potency of pitavastatin has not yet been fully established.
Naturally-occurring statins
Some types of statins are naturally occurring, and can be found in such foods as oyster mushrooms[19] and red yeast rice. Ran nerve study | publisher = USA TODAY | date = 08/20/2002 | url = http://www.usatoday.com/money/markets/2002-08-19-statin_x.htm | accessdate = 2009-10-06 }}</ref> but suggested this side effect is "rare, but it does occur";[20] other researchers have pointed to studies of the effectiveness of statins in trials involving 50,000 people which have not shown nerve damage as a significant side effect.[21]
More serious but rare reactions include myositis and myopathy, with the potential for rhabdomyolysis (the pathological breakdown of skeletal muscle) leading to acute renal failure. Coenzyme Q10 (ubiquinone) levels are decreased in statin use;[22] Q10 supplements are sometimes used to treat statin-associated myopathy, though evidence of their effectiveness is currently lacking.[23] A common variation in the SLCO1B1 gene, which participates in the absorption of statins, has been shown to significantly increase the risk of myopathy.[24]
Graham et al. (2004) reviewed records of over 250,000 patients treated from 1998 to 2001 with the statin drugs atorvastatin, cerivastatin, fluvastatin, lovastatin, pravastatin, and simvastatin.[25] The incidence of rhabdomyolyis was 0.44 per 10,000 patients treated with statins other than cerivastatin. However, the risk was over tenfold greater if cerivastatin was used, or if the standard statins (atorvastatin, fluvastatin, lovastatin, pravastatin, simvastatin) were combined with fibrate (fenofibrate or gemfibrozil) treatment. Cerivastatin was withdrawn by its manufacturer in 2001.
All commonly used statins show somewhat similar results, however the newer statins, characterized by longer pharmacological half-lives and more cellular specificity, have had a better ratio of efficacy to lower adverse effect rates. The risk of myopathy is lowest with pravastatin and fluvastatin probably because they are more hydrophillic and as a result have less muscle penetration. Lovastatin induces this is not recommended as a result of the increased risk and potential for statin toxicity.
Pharmacogenomics
A 2004 study showed that patients with one of two common single nucleotide polymorphisms (small genetic variations) in the HMG-CoA reductase gene were less responsive to statins.[26]
A 2008 study showed that carriers of the KIF6 genetic mutation were more responsive to statin treatment.[27]
Controversy
Some scientists take a skeptical view of the need for many people to require statin treatment. Given the wide indications for which statins are prescribed, and the declining benefit in groups at lower baseline risk of cardiovascular events, the evidence base for expanded statin use has been questioned by some researchers.[28] A much smaller minority, exemplified by The International Network of Cholesterol Skeptics, question the "lipid hypothesis" itself and argue that elevated cholesterol has not been adequately linked to heart disease. These groups claim that statins are not as beneficial or safe as suggested.[29]
References
- ↑ Julio Alarcon, Sergio Aguila, Patricia Arancibia-Avila, Oscar Fuentes, Enrique Zamorano-Ponce, and Margarita Hernandez (2003). Production and Purification of Statins from Pleurotus ostreatus (Basidiomycetes) Strains. Z. Naturforsch. 58c: 62–64.
- ↑ Endo A (1 November 1992). The discovery and development of HMG-CoA reductase inhibitors. J. Lipid Res. 33 (11): 1569–82.
- ↑ Miettinen TA (March 1982). Diurnal variation of cholesterol precursors squalene and methyl sterols in human plasma lipoproteins. Journal of Lipid Research 23 (3): 466–73.
- ↑ Saito Y; Yoshida S; Nakaya N; Hata Y; Goto Y (Jul-Aug 1991). Comparison between morning and evening doses of simvastatin in hyperlipidemic subjects. A double-blind comparative study. Arterioscler Thromb 11.
- ↑ Wallace A; Chinn D; Rubin G (4 October 2003). Taking simvastatin in the morning compared with in the evening: randomised controlled trial. British Medical Journal 327.
- ↑ Cilla DD Jr; Gibson DM; Whitfield LR; Sedman AJ (July 1996). Pharmacodynamic effects and pharmacokinetics of atorvastatin after administration to normocholesterolemic subjects in the morning and evening 36.
- ↑ Ma PT, Gil G, Südhof TC, Bilheimer DW, Goldstein JL, Brown MS (1986). Mevinolin, an inhibitor of cholesterol synthesis, induces mRNA for low density lipoprotein receptor in livers of hamsters and rabbits. Proc. Natl. Acad. Sci. U.S.A. 83 (21): 8370–4. Full text at PMC: 386930
- ↑ Ridker PM, Danielson E, Fonseca FAH, et al. (2008). Rosuvastatin to prevent vascular events in men and women with elevated C-reactive protein. NEJM 359 (21): 2195–207.
- ↑ Cholesterol Drugs May Protect Prostate, Sex Potency, Study Says, Bloomberg, 2009-04-26
- ↑ Law MR, Wald NJ, Rudnicka AR (June 2003). Quantifying effect of statins on low density lipoprotein cholesterol, ischaemic heart disease, and stroke: systematic review and meta-analysis. BMJ 326 (7404): 1423.
- ↑ Wilson P, D'Agostino R, Levy D, Belanger A, Silbershatz H, Kannel W (19 May 1998). Prediction of coronary heart disease using risk factor categories. Circulation 97 (18): 1837–47.
- ↑ Nissen S, Nicholls S, Sipahi I, Libby P, Raichlen J, Ballantyne C, Davignon J, Erbel R, Fruchart J, Tardif J, Schoenhagen P, Crowe T, Cain V, Wolski K, Goormastic M, Tuzcu E (2006). Effect of very high-intensity statin therapy on regression of coronary atherosclerosis: the ASTEROID trial. JAMA 295 (13): 1556–65.
- ↑ Kodach LL, Bleuming SA, Peppelenbosch MP, Hommes DW, van den Brink GR, Hardwick JC. The effect of statins in colorectal cancer is mediated through the bone morphogenetic protein pathway. Gastroenterology 2007 133:1272-81. | PMID: 17919499 |
- ↑ Wolozin, B, Wang SW, Li NC, Lee A, Lee TA, Kazis LE (July 19, 2007). Simvastatin is associated with a reduced incidence of dementia and Parkinson's disease. BMC Medicine 5: 20. Full text at PMC: 1955446
- ↑ Khurana, V, Bejjanki HR, Caldito G, Owens MW (May 2007). Statins reduce the risk of lung cancer in humans: a large case-control study of US veterans. Chest 131 (5): 1282–1288.
- ↑ Klein BE, Klein R, Lee KE, Grady LM (June 2006). Statin use and incident nuclear cataract. JAMA 295 (23): 2752–8.
- ↑ Golomb BA, Dimsdale JE, White HL, Ritchie JB, Criqui MH (April 2008). Reduction in blood pressure with statins: results from the UCSD Statin Study, a randomized trial. Arch. Intern. Med. 168 (7): 721–7.
- ↑ Shepherd J, Hunninghake DB, Barter P, McKenney JM, Hutchinson HG (2003). Guidelines for lowering lipids to reduce coronary artery disease risk: a comparison of rosuvastatin with atorvastatin, pravastatin, and simvastatin for achieving lipid-lowering goals. Am. J. Cardiol. 91 (5A): 11C–17C; discussion 17C–19C.
- ↑ Gunde-Cimerman N, Cimerman A. (Mar 1995). Pleurotus fruiting bodies contain the inhibitor of 3-hydroxy-3-methylglutaryl-coenzyme A reductase-lovastatin.. Exp Mycol. 19 (1): 1–6.
- ↑ includeonly>Sandra G. Boodman, The Washington Post. "Study links statins to nerve damage", Pittsburgh Post-Gazette, September 10, 2002. Retrieved on 2009-10-06.
- ↑ includeonly>Julie Appleby and Steve Sternberg. "Statin side effect rare, but be aware", USA TODAY, 2008. Retrieved on 2009-10-06.
- ↑ Ghirlanda G, Oradei A, Manto A, Lippa S, Uccioli L, Caputo S, Greco A, Littarru G (1993). Evidence of plasma CoQ10-lowering effect by HMG-CoA reductase inhibitors: a double-blind, placebo-controlled study. J Clin Pharmacol 33 (3): 226–9.
- ↑ Marcoff L, Thompson PD (2007). The role of coenzyme Q10 in statin-associated myopathy: a systematic review. J. Am. Coll. Cardiol. 49 (23): 2231–7.
- ↑ (July 2008)SLCO1B1 Variants and Statin-Induced Myopathy -- A Genomewide Study. N. Engl. J. Med. Online (8): 789.
- ↑ Graham DJ, Staffa JA, Shatin D, et al. (2004). Incidence of hospitalized rhabdomyolysis in patients treated with lipid-lowering drugs. JAMA 292 (21): 2585–90.
- ↑ Chasman DI, Posada D, Subrahmanyan L, Cook NR, Stanton VP, Ridker PM (2004). Pharmacogenetic study of statin therapy and cholesterol reduction. JAMA 291 (23): 2821–7.
- ↑ Iakoubova O, Marc S. Sabatine, Charles M. Rowland, et al. Polymorphism in KIF6 Gene and Benefit From Statins After Acute Coronary Syndromes. Journal of the American College of Cardiology. 2008; 51(4): 449-455.
- ↑ Abramson J, Wright J (2007). Are lipid-lowering guidelines evidence-based?. Lancet 369 (9557): 168–9.
- ↑ Ravnskov U, Rosch P, Sutter M, Houston M (2006). Should we lower cholesterol as much as possible?. BMJ 332 (7553): 1330–2.
External links
- Statin page at Bandolier, an evidence-based medicine journal
Pharmacology: major drug groups | |
|---|---|
| Gastrointestinal tract/metabolism (A) |
stomach acid (Antacids, H2 antagonists, Proton pump inhibitors) • Antiemetics • Laxatives • Antidiarrhoeals/Antipropulsives • Anti-obesity drugs • Anti-diabetics • Vitamins • Dietary minerals |
| Blood and blood forming organs (B) |
Antithrombotics (Antiplatelets, Anticoagulants, Thrombolytics/fibrinolytics) • Antihemorrhagics (Platelets, Coagulants, Antifibrinolytics) |
| Cardiovascular system (C) |
cardiac therapy/antianginals (Cardiac glycosides, Antiarrhythmics, Cardiac stimulants) Antihypertensives • Diuretics • Vasodilators • Beta blockers • Calcium channel blockers • renin-angiotensin system (ACE inhibitors, Angiotensin II receptor antagonists, Renin inhibitors) Antihyperlipidemics (Statins, Fibrates, Bile acid sequestrants) |
| Skin (D) |
Emollients • Cicatrizants • Antipruritics • Antipsoriatics • Medicated dressings |
| Genitourinary system (G) |
Hormonal contraception • Fertility agents • SERMs • Sex hormones |
| Endocrine system (H) |
Hypothalamic-pituitary hormones • Corticosteroids (Glucocorticoids, Mineralocorticoids) • Sex hormones • Thyroid hormones/Antithyroid agents |
| Infections and infestations (J, P, QI) |
Antimicrobials: Antibacterials (Antimycobacterials) • Antifungals • Antivirals • Antiparasitics (Antiprotozoals, Anthelmintics, Ectoparasiticides) • IVIG • Vaccines |
| Malignant disease (L01-L02) |
Anticancer agents (Antimetabolites, Alkylating, Spindle poisons, Antineoplastic, Topoisomerase inhibitors) |
| Immune disease (L03-L04) |
Immunomodulators (Immunostimulants, Immunosuppressants) |
| Muscles, bones, and joints (M) |
Anabolic steroids • Anti-inflammatories (NSAIDs) • Antirheumatics • Corticosteroids • Muscle relaxants • Bisphosphonates |
| Brain and nervous system (N) |
Analgesics • Anesthetics (General, Local) • Anorectics • Anti-ADHD Agents • Antiaddictives • Anticonvulsants • Antidementia Agents • Antidepressants • Antimigraine Agents • Antiparkinson's Agents • Antipsychotics • Anxiolytics • Depressants • Entactogens • Entheogens • Euphoriants • Hallucinogens (Psychedelics, Dissociatives, Deliriants) • Hypnotics/Sedatives • Mood Stabilizers • Neuroprotectives • Nootropics • Neurotoxins • Orexigenics • Serenics • Stimulants • Wakefulness-Promoting Agents |
| Respiratory system (R) |
Decongestants • Bronchodilators • Cough medicines • H1 antagonists |
| Sensory organs (S) | |
| Other ATC (V) |
Antidotes • Contrast media • Radiopharmaceuticals • Dressings |
Template:Statins
| This page uses Creative Commons Licensed content from Wikipedia (view authors). |