Assessment |
Biopsychology |
Comparative |
Cognitive |
Developmental |
Language |
Individual differences |
Personality |
Philosophy |
Social |
Methods |
Statistics |
Clinical |
Educational |
Industrial |
Professional items |
World psychology |
Clinical: Approaches · Group therapy · Techniques · Types of problem · Areas of specialism · Taxonomies · Therapeutic issues · Modes of delivery · Model translation project · Personal experiences ·

{kind=link}
The Greek letter Psi is often used as a symbol of psychology.
Clinical psychology is the study and application of psychology for the purpose of understanding, preventing, and relieving psychologically-based distress or dysfunction and to promote subjective well-being and personal development. In many countries it is a regulated mental health profession.
The term was introduced in a 1907 paper by the American psychologist Lightner Witmer, who specifically defined it as the study of individuals, by observation or experimentation, with the intention of promoting change.[1] The modern American Psychological Association offers a more comprehensive definition:[2]
- "The field of Clinical Psychology integrates science, theory, and practice to understand, predict, and alleviate maladjustment, disability, and discomfort as well as to promote human adaptation, adjustment, and personal development. Clinical Psychology focuses on the intellectual, emotional, biological, psychological, social, and behavioral aspects of human functioning across the life span, in varying cultures, and at all socioeconomic levels."
Although different countries require various educational qualifications to practice clinical psychology, it has traditionally required a Doctorate degree—such as the PhD or PsyD in America[1] or the DClinPsy in Britain—although the U.S. now has accredited Masters-level programs as well. U.S. licenses are determined by individual states, and generally reflect the level of education. While doctoral practitioners may qualify for the title of Psychologist, common licenses open to Masters-level graduates include Marriage and Family Therapist (MFT), Licensed Professional Counselor (LPC), and Licensed Psychological Associate. (LPA).
Clinical psychology includes a wide range of practices, such as research, psychological assessment, teaching, consultation, forensic testimony, and program development and administration.[3] Central to clinical psychology is the practice of psychotherapy, which aims to help clients improve subjective well-being, mental health, and life functioning by changing distressing or detrimental thoughts, feelings, or behaviors. Although there are dozens of individual forms of psychotherapy, the three major orientations include psychodynamic, cognitive-behavioral therapy (CBT), and humanistic, although there is a growing movement to integrate these and other approaches resulting in a more eclectic practice. Clinical psychologists can work with individuals, couples, children, older adults, families, small groups, and communities. They may work individually or in multi-disciplinary teams involving other professionals, such as social workers, psychiatrists, and clinical dieticians.
History

{kind=link}
Lightner Witmer, the father of clinical psychology.
- See also: History of psychology
Clinical psychology developed partly as a result of a need for additional clinicians to treat mental health problems, and partly as psychological science advanced to the stage where the fruits of psychological research could be applied in clinical settings. The modern field began with Witmer's establishment of the first psychological clinic in 1896 at the University of Pennsylvania.[4] He also founded the first journal of clinical psychology, Psychological Clinic.
Witmer's call for clinical involvement by psychologists was slow to gain acceptance, but there were twenty-six more clinics in the U.S. by 1914.[5] While Witmer focused on individuals with intellectual deficits, others focused on those in mental distress, and clinical psychology was developing in mental hospitals as psychologists gained staff positions, often working alongside psychiatrists.[6]
In the early 20th century, the psychoanalytic work of Sigmund Freud and Josef Breuer gave great impetus to psychological understandings of mental distress and disorder. However, clinical psychologists did not engage in psychotherapy—a practice that was limited to psychiatrists (i.e. those with a medical degree). Rather, they focused mostly on psychological assessment, and this aspect of early clinical psychology came fully into its own during World War I when the U.S. military required clinical psychologists to assess thousands of new soldiers.[4]
Clinical psychologists began to organize under that name in 1917 with the founding of the American Association of Clinical Psychology, although that organization was soon superseded by the Section on Clinical Psychology of the American Psychological Association.[5] Although psychologists in this section did not qualify for full membership in APA, it did serve to certify them until 1927. Growth in the field was slow for the next few years as various unconnected psychological organizations came together as the American Association of Applied Psychology in 1930. The AAAP became the central organization for applied psychology until 1945 when the APA created what is now called Division 12, its division of clinical psychology.
The assessment-only focus of clinical psychology changed during World War II when the military gave greater recognition to the condition they termed "shell shock" (now called Post Traumatic Stress Disorder or PTSD).[4] The need for treatment was such that military called upon clinical psychologists to assist.
After WWII, a similar problem was faced when tens of thousands of soldiers came home needing psychological care.[7] To meet this challenge, the Veterans Administration made an enormous investment to set up programs to train doctoral-level clinical psychologists. As a consequence, the U.S. went from having no formal university programs in clinical psychology in 1946 to over half of all PhDs in psychology in 1950 being awarded in clinical psychology.[1] As a result of this shift, a report was drafted in 1947 that led to the scientist/practitioner model of clinical psychology, known today as the Boulder Model. This model of graduate training maintained the science and research-oriented focus of the field while adding training in psychotherapy.[5] Similar organizational and theoretical developments took place in other countries in the 1950s, and the number of clinical psychologists proliferated.
In 1973, the Practitioner-Scholar Model of Clinical Psychology—or Vail Model—resulting in the Doctor of Psychology (PsyD) degree was recognized by the Vail Conference on models of training in clinical psychology.[8] At this conference, it was argued that the field of psychology had grown to a degree warranting training persons explicitly in the clinical practice of psychology. Although training would continue to include research skills and a scientific understanding of psychology, the intent would be to produce highly trained professionals, similar to programs in medicine, dentistry, and law. The first pilot PsyD program was instituted at the University of Illinois in 1968, followed by Hahnemann University in 1970 (moved to Widener University in 1989) and Baylor University in 1971.[9] PsyD programs now train about half of all clinical psychologists.
History of psychotherapy
- See also: Timeline of psychotherapy

{kind=link}
Alfred Adler created Individual psychology, one of the first major variations on Freud's Psychoanalysis, and a precursor to Humanistic psychology.
Even as Freud was developing psychoanalysis in the early 1900s theorists began to introduce new conceptions about psychological functioning and change. Early developers of Freud's basic orientation included Alfred Adler, Carl Jung, and even his own daughter, Anna. These and other theorists helped to develop the general orientation now called psychodynamic therapy, which includes the various therapies based on Freud's essential principle of making the unconscious conscious.
In the 1920s, behaviorism became the dominant paradigm within the general field, and remained so until the 1950s. Major contributors were Joseph Wolpe, Hans Eysenck, and B.F. Skinner. Behavioral therapy approaches relied on principles of operant conditioning, classical conditioning and social learning theory to bring about therapeutic change in observable symptoms. Because behaviorism denied or ignored internal mental activity, this period represents a general slowing of advancement within the field of psychotherapy.[4]
Starting in the 1950s, two main orientations evolved independently in response to behaviorism—cognitivism and humanistic therapy.[7] The former reestablished an interest in cognition (i.e. mental processes and experiences) and the latter ignited renewed interest in human well-being and improvement. The humanistic movement largely developed from both the Existential theories of writers like Rollo May and Viktor Frankl and the Person-centered psychotherapy of Carl Rogers. This orientation focused less on the unconscious and more on promoting positive, holistic change through the development of a supportive, genuine, and empathic therapeutic relationship. An influential psychotherapy that came out of this movement was Gestalt therapy developed by Fritz and Laura Perls in the 1940s-50s.
During the 1960s, Albert Ellis developed Rational Emotive Behavior Therapy (REBT). Around the same time, psychiatrist Aaron T. Beck developed a form of psychotherapy known as cognitive therapy. Both of these included short, structured and present-focused therapy aimed at changing a person's distorted thinking, by contrast with the long-lasting insight-based approach of psychodynamic therapies or the newer relational approach of humanistic therapies. Cognitive and behavioral therapy approaches were combined during the 1970s, resulting in Cognitive behavioral therapy (CBT).[7] Being oriented towards symptom-relief, collaborative empiricism and modifying peoples core beliefs, the approach gained widespread acceptance as a primary treatment for numerous disorders. A "third wave" of cognitive and behavioral therapies developed, including Acceptance and Commitment Therapy and Dialectical behavior therapy, which expanded the concepts to other disorders and/or added novel components.
Since the 1970s, other major perspectives have been developed and adopted within the field. Perhaps the two biggest have been Systems Therapy—which focuses on family and group dynamics—and Transpersonal psychology, which focuses on the spiritual facet of human experience. Other important orientations developed in the last three decades include Feminist therapy, Narrative therapy, Brief therapy, Somatic Psychology, Expressive therapy, and applied Positive Psychology.
With the advent of more robust research findings regarding psychotherapy, there is growing evidence that most of the major therapies are about of equal effectiveness (although the most evidence for it belongs to CBT).[10][11] Because of this, more training programs and psychologists are adopting an eclectic orientation. This integrative movement attempts to combine the most effective aspects of all the schools of practice, giving clinicians a wider range of options for treatment.
Training


{kind=link}
The University of Pennsylvania was the first to offer formal education in clinical psychology.
Doctoral level training
Clinical psychologists undergo many hours of graduate training—usually 4 to 6 years post-Bachelors—in order to gain demonstrable competence and experience. Today, in America, about half of all clinical psychology graduate students are being trained in PhD programs—a model that emphasizes research and is usually housed in universities—with the other half in PsyD programs, which has more focus on practice (similar to professional degrees for medicine and law).[8] Both models envision practicing Clinical Psychology in a research-based, scientifically valid manner, and are accredited by the American Psychological Association[12] and many other English-speaking psychological societies.
Doctorate (PhD and PsyD) programs usually involve some variation on the following 4 to 6 year, 90-unit curriculum:
- Bases of behavior—biological, cognitive-affective, and cultural-social
- Individual differences—personality, lifespan development, psychopathology
- History and systems—development of psychological theories, practices, and scientific knowledge
- Clinical practice—diagnostics, psychological assessment, psychotherapeutic interventions, psychopharmacology, ethical and legal issues
- Clinical experience
- Practicum—usually one or two years of working with clients under supervision in a clinical setting
- Doctoral Internship—usually an intensive one or two year placement in a clinical setting
- Dissertation—PhD programs usually require original quantitative empirical research, while PsyD dissertations often address qualitative research, theoretical scholarship, program evaluation or development, critical literature analysis, or clinical application and analysis
- Specialized electives—many programs offer sets of elective courses for specializations, such as health, child, family, community, or neuropsychology
- Personal psychotherapy—many programs require students to undertake a certain number of hours of personal psychotherapy (with a non-faculty therapist)
Masters level training
| Sample Curriculum for MA in Clinical Psychology in the U.S. | ||
| State Required | School Required | Electives |
|
Chemical Dependency: 3 |
Process and Psychotherapy: 4 |
Gay and Lesbian Issues: 2 |
Where subject is required by both the state and the school, it is shown under the school's required column. Similar courses have been lumped together, for example "Group Treatment Techniques" and "Couples Counseling" were combined, their units added together and called "Group and Couples Treatment"—just to keep the table of manageable size.
There are a number of U.S. schools offering accredited programs in clinical psychology resulting in a Masters degree. Such programs can range from 48 to 84 units, most often taking 2 to 3 years to complete post-Bachelors. Training usually emphasizes theory and treatment over research, quite often with a focus on school or couples and family counseling. Similar to doctoral programs, Masters-level students usually must fulfill time in a clinical practicum under supervision and undergo a minimum amount of personal psychotherapy.[13] While many graduates from Masters-level training go on to doctoral programs, a large number also go directly into practice—often as a Licensed Professional Counselor (LPC), Marriage and Family Therapist (MFT) or other similar license.[14]
Training in Britain
In the U.K., clinical psychologists undertake a DClinPsy (or similar), which is a doctorate with both clinical and research components. This is a three-year full-time salaried program sponsored by the National Health Service (NHS). Entry into these programs is highly competitive, and requires at least a three-year undergraduate degree in psychology approved by the British Psychological Society or an approved conversion course, plus some form of experience, usually in either the NHS as an Assistant Psychologist or in academia as a Research Assistant.[15]
Professional practice
Clinical psychologists can offer a range of professional services, including:[1]
- Provide psychological treatment (psychotherapy)
- Administer and interpret psychological assessment and testing
- Conduct psychological research
- Teaching
- Development of prevention programs
- Consultation (especially with schools and businesses)
- Program administration
- Provide expert testimony (forensics)
In practice, clinical psychologists may work with individuals, couples, families, or groups in a variety of settings, including private practices, hospitals, mental health organizations, schools, businesses, and non-profit agencies. Most clinical psychologists who engage in research and teaching do so within a college or university setting. Clinical psychologists may also choose to specialize in a particular field—common areas of specialization, some of which can earn board certification,[16] include:
Comparison with other mental health professions
Psychiatry
- Main article: Psychiatry

{kind=link}
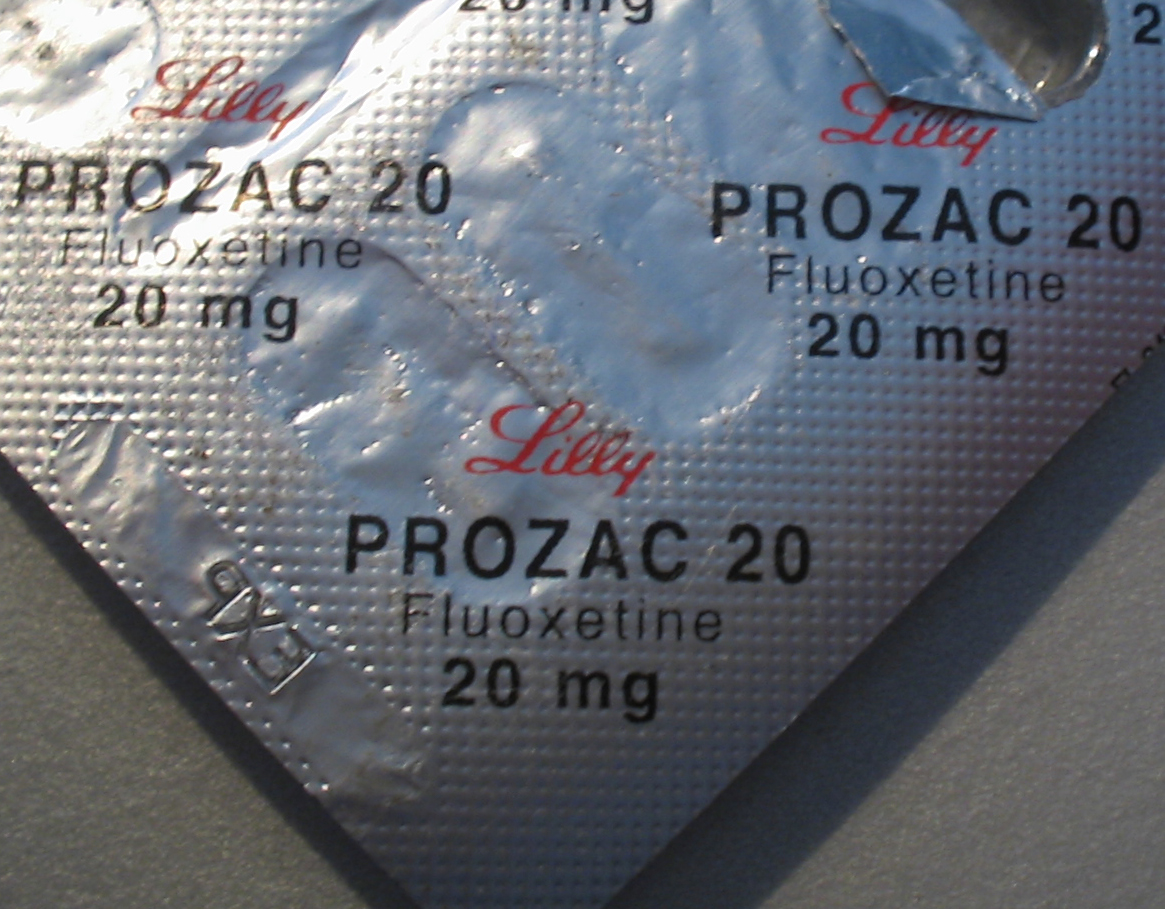
Fluoxetine hydrochloride, branded by Lilly as Prozac, is a common antidepressant drug prescribed by psychiatrists. There is a growing movement to give prescription privileges to qualified psychologists.
Although clinical psychologists and psychiatrists share the same fundamental aim—the alleviation of mental distress—their training, outlook, and methodologies are often quite different. Perhaps the most significant difference is that psychiatrists are medical doctors with four years of medical school and another four years of residency in a medical setting where they can often choose to specialize, such as working with children or people with specific conditions. Being medical doctors, they tend to use the medical model to assess psychological problems (i.e. those they treat are seen as patients with an illness) and rely on psychotropic medications as the chief method of addressing them[17]—although many also employ psychotherapy as well. Their medical training does give them an advantage in terms of being able to conduct physical examinations, order and interpret laboratory tests and EEGs, and may order brain imaging studies such as CT or CAT, MRI, and PET scanning.
Clinical psychologists do not usually prescribe medication, although there is a growing movement for psychologists to have limited prescribing privileges.[18] Such privileges require additional, supervised training and education, and would mostly be limited to psychotropic medications. To date, qualified psychologists may prescribe psychotropic medications in Guam, New Mexico, and Louisiana.[19] In general, however, when medication is warranted many psychologists will work in cooperation with psychiatrists so that clients get all their therapeutic needs met.[3]
Unless a psychiatrist voluntarily chooses to get extra training, such as at a psychoanalytic institute, they will have less training in the theory and practice of psychotherapy than will a licensed clinical psychologist.[20] Even though many psychiatrists do seek out such training, the majority of them increasingly focus on medication management, possibly because insurance tends to pay far more for this service than for psychotherapy.[21] Further, psychologists tend to have more training in psychological assessment.
Counseling psychology
- Main article: Counseling Psychology
Counseling generally involves helping people with what might be considered "normal" or "moderate" psychological problems, such as the feelings of anxiety or sadness resulting from major life changes or events.[3][1] As such, counseling psychologists often help people adjust to or cope with their environment or major events, although many also work with more serious problems as well. Clinical psychologists, by comparison, are trained to help with these kinds of issues but also more debilitating or chronic problems, such as forms of dementia or psychosis. Other differences include: there are fewer counseling psychology graduate programs, they are usually housed in departments of education (as opposed to psychology departments for clin-psy programs), counseling psychologists tend to conduct more vocational assessment and less projective or objective assessment, and they are more likely to work in public service or university clinics (compared with clinical psychologists who are more likely to work in hospitals or private practice).[22] Despite these differences, there is considerable overlap between the two fields and distinctions between them continue to fade.
School psychology
- Main article: School psychology
School psychologists' primary concern is with the academic, social, and emotional well-being of children within a scholastic environment. Unlike clinical psychologists, they receive much more training in education, child development and behavior, and the psychology of learning, often graduating with a post-Masters Educational Specialist Degree (EdS) or Doctor of Education (EdD) degree. Besides offering individual and group therapy with children and their families, school psychologists also evaluate school programs, provide cognitive assessment, help design prevention programs (e.g. reducing drops outs), and work with teachers and administrators to help maximize teaching efficacy, both in the classroom and systemically.[23]
Social Workers
Main article: Social Work
Social Workers provide a variety of services, including psychology, in a clinical setting . This might be done on behalf of a mental health clinic, a private practice, Federal Government, in a school setting, a social welfare agency, a hospital or for a department of social services.
Clinical Social Work Defined American Board of Examiners in Clinical Social Work (ABE)
Clinical social work is a practice specialty of the social work profession. It builds upon generic values, ethics, principles, practice methods, and the person-in-environment perspective of the profession. Its purposes are to:
Diagnose and treat bio-psycho-social disability and impairment, including mental and emotional disorders and developmental disabilities. Achieve optimal prevention of bio-psycho-social dysfunction. Support and enhance bio-psycho-social strengths and functioning. Clinical social work practice applies specific knowledge, theories, and methods to assessment and diagnosis, treatment planning, intervention, and outcome evaluation. Practice knowledge incorporates theories of biological, psychological, and social development. It includes, but is not limited to, an understanding of human behavior and psychopathology, human diversity, interpersonal relationships and family dynamics; mental disorders, stress, chemical dependency, interpersonal violence, and consequences of illness or injury; impact of physical, social, and cultural environment; and cognitive, affective, and behavioral manifestations of conscious and unconscious processes.
Clinical social work interventions include, but are not limited to, assessment and diagnosis, crisis intervention, psychosocial and psychoeducational interventions, and brief and long-term psychotherapies. These interventions are applied within the context of professional relationships with individuals, couples, families, and groups. Clinical social work practice includes client-centered clinical supervision and consultation with professional colleagues.
Adopted 12 Feb. 1995 All rights reserved.
The Master's in Clinical Social Work is a two-year (at times three year) eighty credit program that must also include a full two year concurrent practicum. Unlike the Ph.D., which is an academic degree mainly for teaching and testing, the M.S.W. is considered a professional clinical degree. License requires a Doctorate (DSW/PhD) or Masters degree (MSW). In addition, it usually involves 3200 hours & at least 2 years of post-degree clinical experience under supervision, and licensure requires passing both a written as well as oral exam to obtain, Licensed Clinical Social Worker (LCSW).
Licensure
The practice of clinical psychology requires a license in the United States, Canada, the United Kingdom, and many other countries. Although each of the U.S. states is somewhat different in terms of requirements and licenses (see [2] and [3] for examples), there are three common elements:[24]
- Graduation from an accredited school with the appropriate degree
- Completion of supervised clinical experience
- Passing a written examination and, in some states, an oral examination
| Clinical Psychologists and other mental health professionals | ||||
| Occupation | Degree | Common Licenses | Prescription Privilege | Ave. 2004 Income |
| Clinical Psychologist | PhD/PsyD | Psychologist | Mostly no | $75,000 |
| Counselor/Psychotherapist (Doctorate) | PhD | MFT/LPC | No | $65,000 |
| School Psychologist | EdD | LEP | No | $78,000 |
| Counselor/Psychotherapist (Masters) | MA/MS/MC | MFT/LPC/LPA | No | $49,000 |
| Psychiatrist | MD/DO | Psychiatrist | Yes | $145,600 |
| Clinical Social Worker | PhD/MSW | LCSW | No | $51,500 |
| Psychiatric Nurse | PhD/MSN/BSN | APRN/PMHN | No | $53,450 |
| Psychiatric and mental health Nurse Practitioner | DNP/MSN | MHNP | Yes (Varies by state) | $75,711 |
| Expressive/Art Therapist | MA | ATR | No | $45,000 |
All U.S. state and Canada province licensing boards are members of the Association of State and Provincial Psychology Boards (ASPPB) which created and maintains the Examination for Professional Practice in Psychology (EPPP). Many states require other examinations in addition to the EPPP, such as a jurisprudence (i.e. mental health law) examination and/or an oral examination.[24] Most states also require a certain number of continuing education credits per year in order to renew a license, which can be obtained though various means, such as taking audited classes and attending approved workshops.
There are several licenses that allow one to practice clinical psychology, usually awarded in relation to one's educational degree.
- Psychologist. To practice with the title of Psychologist, in almost all cases a Doctorate degree is required (a PhD or PsyD in the U.S.). Normally, after the degree, the practitioner must fulfill a certain number of supervised postdoctoral hours (usually taking 1 to 2 years), and passing the EPPP and any other provincial exams.[31]
- Marriage and Family Therapist (MFT). An MFT license requires a Doctorate or Masters degree. In addition, it usually involves 2 years of post-degree clinical experience under supervision, and licensure requires passing a written exam, commonly the National Examination for Marriage and Family Therapists which is maintained by the American Association for Marriage and Family Therapy. In addition, most states require an oral exam. MFTs, as the title implies, work mostly with families and couples, addressing a wide range of common psychological problems.[32]
- Licensed Professional Counselor (LPC). Similar to the MFT, the LPC license requires a Masters or Doctorate degree, a minimum number of hours of supervised clinical experience in a pre-doc practicum, and the passing of the National Counselor Exam. Similar licenses are the Licensed Mental Health Counselor (LMHC), Licensed Clinical Professional Counselor (LCPC), and Clinical Counselor in Mental Health (CCMH). In some states, after passing the exam, a temporary LPC license is awarded and the clinician may begin the normal 3000-hour supervised internship leading to the full license allowing for the practice as a counselor or psychotherapist, usually under the supervision of a licensed psychologist.[33]
- Licensed Psychological Associate. (LPA) About twenty-six states offer a Masters-only license, a common one being the LPA, which allows for the therapist to either practice independently or (more commonly) under the supervision of a licensed psychologist, depending on the state.[14] Common requirements are 2 to 4 years of post-Masters supervised clinical experience and passing a Psychological Associates Examination. Other titles for this level of licensing include Psychological Technician (Alabama), Psychological Assistant (California), Licensed Clinical Psychotherapist (Kansas), Licensed Psychological Practitioner (Minnesota), Licensed Behavioral Practitioner (Oklahoma), or Psychological Examiner (Tennessee).
In the U.K., many mental health titles, including "psychologist", are not protected—although statutory registration of all the mental health professions is planned in the near future to help the public know who is qualified to practice. Currently, protected titles include "clinical psychologist", "counselling psychologist", and "educational psychologist". One can also become "Chartered" by the British Psychological Society. The title of "Assistant Psychologist" is used by a psychology graduate under the supervision of a qualified clinical psychologist, and the title "Trainee Clinical Psychologist" is used during the three-year doctoral program.
Assessment
- Main article: Psychological testing
An important area of expertise for many clinical psychologists is psychological assessment, and there are indications that as many as 91% of psychologists engage in this core clinical practice.[34] Such evaluation is usually done in service to gaining insight into and forming hypotheses about psychological or behavioral problems. As such, the results of such assessments are usually used to create generalized impressions rather than diagnoses.
There exists literally hundreds of various assessment tools, although only a few have been shown to have both high validity (i.e., test actually measures what it claims to measure) and reliability (i.e., test is consistent—internally, over time, and regardless of administrator). These measures generally fall within one of several categories, including the following:
- Intelligence & achievement tests. These tests are designed to measure certain specific kinds of cognitive functioning (often referred to as IQ) in comparison to a norming-group. Commonly used today are the Weschler tests (the WAIS-III for adults, the WISC-IV for children, and the WIAT-II achievement test), the Woodcock-Johnson-III, and the Stanford-Binet-5. These tests generally measure areas such as verbal skills (e.g. comprehension and vocabulary), memory (short and long term), attention span, arithmetic, and non-verbal performance (e.g. visual/spacial perception, hand-eye coordination, problem solving, and logical reasoning). These tests have been shown to accurately predict certain kinds of performance, especially scholastic.[34]
- Personality tests. Tests of personality aim to describe characteristic patterns of behavior, thoughts, and feelings that remain relatively stable throughout a person's lifetime. They generally fall within two categories: objective (offering restricted, measured responses, such as yes/no, true/false, or a rating scale) and projective (which allow a person to respond to ambiguous stimuli, presumably revealing non-conscious psychological dynamics). Typical objective tests used today are the Minnesota Multiphasic Personality Inventory, the Millon Clinical Multiaxial Inventory-III, and the California Psychological Inventory. Common projective tests include the Rorschach inkblot test and the Thematic Apperception Test.
- Neuropsychological tests. Neuropsychological tests consist of specifically designed tasks used to measure psychological functions known to be linked to a particular brain structure or pathway. They are typically used to assess impairment after an injury or illness known to affect neurocognitive functioning, or when used in research, to contrast neuropsychological abilities across experimental groups. Examples include the Stroop test, the Bender-Gestalt Test, the Trail Making task, and finger tapping.
- Clinical observation. Clinical psychologists are also trained to gather data by observing behavior. The clinical interview is a vital part of assessment, even when using other formalized tools, which can employ either a structured or unstructured format. Such assessment looks at certain areas, such as general appearance and behavior, mood and affect, perception, comprehension, orientation, insight, memory, and content of communication. One common example of a formal interview is the mental status examination, which is often used as a screening tool for treatment or further testing.[34]
Diagnostic impressions

{kind=link}
The Diagnostic and Statistical Manual published by the American Psychiatric Association.
After assessment, clinical psychologists often provide a diagnostic impression. In the U.S., many psychologists use the Diagnostic and Statistical Manual of Mental Disorders (the DSM version IV-TR)—especially when working with an HMO or insurance company—whereas many other countries are more likely to use the International Statistical Classification of Diseases and Related Health Problems. Both assume medical concepts and terms, and state that there are categorical disorders that can be diagnosed by set lists of criteria, which serves psychologists by providing a familiar frame of reference for discussing and understanding the clinical experience and for guiding treatment.[35]
The DSM organizes psychological disorders in five axes:
- Axis I: Clinical disorders; Other conditions that may be a focus of clinical attention
- Typical disorders include autism, ADHD, dementia, substance abuse, schizophrenia, depression, bipolar, phobias, PTSD, amnesia, anorexia, insomnia, and adjustment disorder
- Axis II: Personality disorders (generally rigid and self-defeating traits that are persistent over time and affect day to day living)
- Typical disorders include obsessive-compulsive PD, paranoid PD, borderline PD, and narcissistic PD. Mental retardation is also placed on Axis II.
- Axis III: medical conditions contributing to the disorder
- Axis IV: psychosocial and environmental factors contributing to the disorder
- Axis V: Global Assessment of Functioning (on a scale from 100 to 0)
The DSM uses a categorical medical model and views psychological problems in terms of discrete illnesses that can be defined by a minimum set of criteria (such as presenting problems, intensity, behaviors, duration, onset, etc.). While convenient for prescribing medications, there is a growing awareness that this model is not the only way to understand psychological functioning and the various causes of mental distress. Moreover, there is little justification for the cutoff criteria, which, except for schizotypal and borderline diagnoses, are essentially arbitrary.[36] As such, there are many debates in the field regarding alternative methods of diagnosing psychological problems.
One such debate is the position of adopting a dimensional model which could be based on empirically validated models of human differences, such as the five factor model of personality. A dimensional model would arguably have several major advantages, including—addressing quantitative variation and shifts (between various disorders as well as between what is considered normal and pathological); dealing with co-occurrence of multiple problems; and a more constructive way of looking at otherwise 'sub-threshold' conditions.[36][35]
Another variation is called the psychosocial model, which could be more relevant for the practice of psychotherapy (as opposed to medicine).[37] While the medical model of the DSM is based on assumptions of biology, stability of diagnosis, and objective traits, the psychosocial model is more psychological, intersubjective, and diagnostically flexible over the course of therapy.
British clinical psychologists do not tend to diagnose, but rather use formulation—an individualized map of the difficulties that the patient or client faces, encompassing predisposing, precipitating and perpetuating (maintaining) factors.[38]
Psychotherapy

{kind=link}
Clinical psychologists work with individuals, children, families, couples, or small groups.
- Main article: Psychotherapy
The central intervention used by clinical psychologists is psychotherapy, which uses a wide range of techniques to change thoughts, feelings, or behaviors in service to enhancing subjective well-being, mental health, and life functioning. Generally speaking, psychotherapy involves a formal relationship between professional and client—usually an individual, couple, family, or small group—that employs a set of procedures intended to form a therapeutic alliance, explore the nature of psychological problems, and encourage new ways of thinking or behaving.
Although there are literally dozens of recognized therapeutic orientations, their differences can often be categorized on two dimensions: insight vs. action and in-session vs. out-session.[1]
- Insight—emphasis is on gaining greater understanding of the motivations underlying one's thoughts and feelings (e.g. Psychodynamic therapy)
- Action—focus is on making changes in how one thinks and acts (e.g. Cognitive Behavioral Therapy)
- In-session—interventions center on the here-and-now interactions between client and therapist (e.g. Humanistic therapy)
- Out-session—although the importance of the relationship is recognized, therapy is geared towards helping the client make changes outside of the session (e.g. Rational Emotive Behavior Therapy)
The methods used are also different in regards to the population being served as well as the context and nature of the problem. Therapy will look very different between, say, a traumatized child, a depressed but high-functioning adult, a group of people recovering from substance dependence, and a ward of the state suffering from terrifying delusions. Other elements that play a critical role in the process of psychotherapy include the environment, culture, age, cognitive functioning, motivation, and duration (i.e. brief or long-term therapy).
The Big Three perspectives
The field generally recognizes three major perspectives regarding the practice of clinical psychology: Psychodynamic, Cognitive Behavioral, and Humanistic (while a growing debate exists about including the Transpersonal perspective, which recognizes a spiritual dimension in psychological well-being).[39]


{kind=link}
Sigmund Freud, founder of Psychoanalysis.
Psychodynamic
- Main article: Psychodynamic psychotherapy
The Psychodynamic perspective developed out of the Psychoanalysis of Sigmund Freud (which is still practiced in its orthodox form). The core object of Psychoanalysis is to make the unconscious conscious—to make the client aware of his or her own primal drives (namely those relating to sex and aggression) and the various defenses used to keep them in check. The essential tools of the psychoanalytic process are the use of free association and an examination of the client's transference towards the therapist, defined as the tendency to take unconscious thoughts or emotions about a significant person (e.g. a parent) and "transfer" them onto another person.[40]
Many theorists built upon Freud's fundamental ideas, including Anna Freud, Alfred Adler, Carl Jung, Karen Horney, Erik Erikson, Melanie Klein, and Heinz Kohut. Major variations on Freudian psychoanalysis practiced today include Self Psychology, Ego Psychology, and Object Relations Theory. These general orientations now fall under the umbrella term psychodynamic psychology, with common themes including examination of transference and defenses, an appreciation of the power of the unconscious, and a focus on how early developments in childhood have shaped the client's current psychological state.[40]


{kind=link}
Albert Ellis, creator of Rational Emotive Behavior Therapy, a precursor of CBT.
Cognitive Behavioral
- Main article: Cognitive behavioral therapy
Cognitive Behavioral Therapy (CBT) developed from the combination of Cognitive psychology and Behaviorism, largely based on the work of theorists Albert Ellis and Aaron T. Beck in the 1950s and 1960s. Essentially, CBT is based on the idea that how we think (cognition), how we feel (emotion), and how we act (behavior) all interact together. In this perspective, certain thoughts or ways of interpreting the world (called schemas) can cause emotional distress or result in behavioral problems. The object of CBT is to discover the biased and irrational thinking that leads to emotional problems and to help the client take control over his or her thinking processes in such a way that will lead to increased well-being.[41] There are several approaches that fall into the category of CBT, such as Dialectic Behavior Therapy, Systematic Desensitization, and Mindfulness-based Cognitive Therapy[42], all of which have been empirically shown to be effective in treating certain conditions, such as depression and phobias.[43]

{kind=link}
Carl Rogers, therapist who helped establish the Humanistic perspective.
Humanistic
- Main article: Humanistic psychology
Humanistic psychology was developed in the 1950s in reaction to both behaviorism and psychoanalysis, largely due to the Person-Centered Therapy of Carl Rogers (often referred to as Rogerian Therapy). Rogers believed that a client needed only three things from a clinician to experience therapeutic improvement—congruence, unconditional positive regard, and empathetic understanding.[44] The aim of much humanistic therapy is to give a holistic description of the person. By using Phenomenology, Intersubjectivity and first-person categories, the humanistic psychologist hopes to get a glimpse of the whole person and not just the fragmented parts of the personality.[45] This aspect of holism links up with another aim of humanistic psychology, which is to seek an integration of the whole person, also called self-actualization. According to humanistic thinking, each individual person already has inbuilt potentials and resources that might help them to build a stronger personality and self-concept. The mission of the humanistic psychologist is to help the individual employ these resources via the therapeutic relationship.
Other major therapeutic orientations
- See also: List of psychotherapies
There exists literally dozens of recognized schools or orientations of psychotherapy—the list below represents those that have been pivotal in the development of clinical psychology. Although they all have some typical set of techniques practitioners employ, they are generally better known for providing a framework of theory and philosophy that guides a therapist in his or her working with a client.
- Systems or Family Therapy. Systems or Family therapy works with couples and families, and emphasizes family relationships as an important factor in psychological health. The central focus tends to be on interpersonal dynamics, especially in terms of how change in one person will affect the entire system.[46] Therapy is therefore conducted with as many significant members of the "system" as possible. Goals can include improving communication, establishing healthy roles, creating alternative narratives, and addressing problematic behaviors.

{kind=link}
Victor Frankl, founder of Logotherapy, was highly influential in the development of Existential therapy.
- Existential. Existential psychotherapy postulates that people are largely free to choose who we are and how we interpret and interact with the world. It intends to help the client find deeper meaning in life and to accept responsibility for living. As such, it addresses fundamental issues of life, such as death, aloneness, and freedom. The therapist emphasizes the client’s ability to be self-aware, freely make choices in the present, establish personal identity and social relationships, create meaning, and cope with the natural anxiety of living.[47] Important writers in existential therapy include Rollo May, Victor Frankl, and Irvin Yalom.
One influential therapy that came out of Existential therapy is Gestalt Therapy, primarily founded by Fritz Perls in the 1950s. It is well-known for techniques designed to increase various kinds of self-awareness—the best-known perhaps being the empty chair technique—which are generally intended to explore resistance to authentic contact, resolve internal conflicts, and help the client complete "unfinished business".[48]
- Postmodern. Postmodern psychology says that the experience of reality is a subjective construction built upon language, social context, and history, with no essential truths.[49] Since "mental illness" and "mental health" are not recognized as objective, definable realities, the postmodern psychologist instead sees the goal of therapy strictly as something constructed by the client and therapist.[50] Forms of postmodern psychotherapy include Narrative Therapy, Solution-Focused Therapy, and Coherence Therapy.
- Transpersonal. Transpersonal therapy is a relatively new but rapidly growing orientation that places a stronger focus on the spiritual facet of human experience.[51] Similar to Existential therapy, it is not a set of techniques so much as a willingness to help a client explore spirituality and/or transcendent states of consciousness. It also is concerned with helping clients achieve his or her highest potential. Important writers in this area include Ken Wilber, Abraham Maslow, Stanislav Grof, John Welwood, and David Brazier.
Integration
- Main article: Integrative Psychotherapy
In the last couple of decades, there has been a growing movement to integrate the various therapeutic approaches, especially with an increased understanding of cultural, gender, spiritual, and sexual-orientation issues. Clinical psychologists are beginning to look at the various strengths and weaknesses of each orientation while also working with related fields, such as neuroscience, genetics, evolutionary biology, and psychopharmacology. The result is a growing practice of eclecticism, with psychologists learning various systems and the most efficacious methods of therapy with the intent to provide the best solution for any given problem.[52]
Other perspectives
- Multiculturalism. Although the theoretical foundations of psychology are rooted in European culture, there is a growing recognition that there exist profound differences between various ethnic and social groups and that systems of psychotherapy need to take those differences into greater consideration.[53] Further, the generations following immigrant migration will have some combination of two or more cultures—with aspects coming from the parents and from the surrounding society—and this process of acculturation can play a strong role in therapy (and might itself be the presenting problem). Culture influences ideas about change, help-seeking, locus of control, authority, and the importance of the individual versus the group, all of which can potentially clash with certain givens in psychotherapeutic theory and practice.[54] As such, more psychologists and training programs are integrating knowledge of various cultural groups in order to inform therapeutic practice in a more culturally sensitive and effective way.
- Positive Psychology. Positive psychology is the scientific study of human happiness and well-being, which started to gain momentum in 1998 due to the call of Martin Seligman,[55] then president of the APA. The history of psychology shows that the field has been primarily dedicated to addressing mental illness rather than mental wellness. Applied positive psychology's main focus, therefore, is to increase one's positive experience of life and ability to flourish by promoting such things as optimism about the future, a sense of flow in the present, and personal traits like courage, perseverance, and altrusism.[56][57] There is now preliminary empirical evidence to show that by promoting Seligman's three components of happiness—positive emotion (the pleasant life), engagement (the engaged life), and meaning (the meaningful life)—positive therapy can decrease clinical depression.[58]
- Feminism. Feminist therapy is an orientation arising from the disparity between the origin of most psychological theories (which have male authors) and the majority of people seeking counseling being female. It focuses on societal, cultural, and political causes and solutions to issues faced in the counseling process. It openly encourages the client to participate in the world in a more social and political way.[59]
Clinical psychology journals
The following represents an (incomplete) listing of significant journals in the field of clinical psychology.
|
|
Major influences
Criticisms and controversies
- Clinical Psychology is sometimes subject to the criticisms leveled at psychiatry, for example by the anti-psychiatry movement. This may be the case, for example, when using categorical medical diagnoses such as in the DSM—which views the client as having an illness—an attitude that some see as demeaning or disempowering.[How to reference and link to summary or text]
- Clinical Psychologists are sometimes criticized by psychiatrists for not having the same degree of training or knowledge in general medicine or in medication, or as not being as scientific. There has been controversy over attempts by clinical psychologists to obtain prescribing privileges.[60]
- Although some research has offered evidence that most forms of therapy are equally effective, there remains much debate about the efficacy of various forms of treatment (especially humanistic and transpersonal therapies). This debate often extends into the comparison between therapy and medication.[61]
- Alternatively, some methods have been criticized as overly-reductionistic, mechanical, and dehumanizing; for example those originating in behaviorism.[How to reference and link to summary or text]
See also
Related lists
References
- ↑ 1.0 1.1 1.2 1.3 1.4 1.5 Compass, B. & Gotlib, I. (2002). Introduction to Clinical Psychology. New York, NY : McGraw Hill. ISBN 0-07-012491-4
- ↑ American Psychological Association, Division 12, "About Clinical Psychology"
- ↑ 3.0 3.1 3.2 Brain, Christine. (2002). Advanced psychology : applications, issues and perspectives. Cheltenham : Nelson Thornes. ISBN 0174900589>
- ↑ 4.0 4.1 4.2 4.3 Alessandri, M., Heiden, L., & Dunbar-Welter, M. (1995). "History and Overview" in Heiden, Lynda & Hersen, Michel. (eds.), Introduction to clinical psychology. New York : Plenum Press. ISBN 0306448777
- ↑ 5.0 5.1 5.2 Evans, Rand. (1999). Clinical psychology born and raised in controversy. APA Monitor, 30(11).
- ↑ Routh, Donald. (1994). Clinical psychology since 1917 : Science, practice, and organization. New York : Plenum Press. ISBN 0306444526
- ↑ 7.0 7.1 7.2 Reisman, John. (1991). A History of Clinical Psychology. UK : Taylor Francis. ISBN 1560321881
- ↑ 8.0 8.1 Norcross, J. & Castle, P. (2002). Appreciating the PsyD: The Facts. Eye on Psi Chi, 7(1), 22-26.
- ↑ Murray, Bridget. (2000). The degree that almost wasn't: The PsyD comes of age. Monitor on Psychology, 31(1).
- ↑ Leichsenring, Falk & Leibing, Eric. (2003). The effectiveness of psychodynamic therapy and cognitive behavior therapy in the treatment of personality disorders: A meta-analysis. The American Journal of Psychiatry, 160(7), 1223-1233.
- ↑ Reisner, Andrew. (2005). The common factors, empirically validated treatments, and recovery models of therapeutic change. The Psychological Record, 55(3), 377-400.
- ↑ APA. (2005). Guidelines and Principles for Accreditation of Programs in Professional Psychology: Quick Reference Guide to Doctoral Programs.
- ↑ Antioch University. (2006). Master of Arts in Psychology Program Options & Requirements.
- ↑ 14.0 14.1 Northamerican Association of Masters in Psychology. (2004). Licensure Information.
- ↑ Cheshire, K. & Pilgrim, D. (2004). A short introduction to clinical psychology. London ; Thousand Oaks, CA : Sage Publications. ISBN 076194768X
- ↑ American Board of Professional Psychology, Specialty Certification in Professional Psychology
- ↑ Graybar, S. & Leonard, L. (2005). In defense of listening. American Journal of Psychotherapy, 59(1), 1-19.
- ↑ Klusman, Lawrence. (2001). Prescribing Psychologists and Patients' Medical Needs; Lessons From Clinical Psychiatry. Professional Psychology: Research and Practice, 32(5), 496.
- ↑ Halloway, Jennifer. (2004). Gaining prescriptive knowledge. Monitor on Psychology, 35(6). p.22.
- ↑ Mariani, Matthew. (1995). Beyond psychobabble: Careers in psychotherapy. Occupational Outlook Quarterly, 39(1), 12-26.
- ↑ Downs, Martin. (2005). "Psychology vs. Psychiatry: Which Is Better?" WebMD.
- ↑ Norcross, John. (2000). Clinical versus counseling psychology: What's the diff? Eye on Psi Chi, 5(1), 20-22.
- ↑ Silva, Arlene. (2003). Who Are School Psychologists?. National Association of School Psychologists.
- ↑ 24.0 24.1 Association of State and Provincial Psychology Boards. URL accessed on 2007-02-17.
- ↑ APA. (2003). Salaries in Psychology 2003: Report of the 2003 APA Salary Survey
- ↑ NIH: Office of Science Education. (2006). Lifeworks: Psychiatrist
- ↑ U.S. Department of Labor: Bureau of Labor Statistics. (2004). Occupational Outlook Handbook: Social Workers
- ↑ U.S. Department of Labor: Bureau of Labor Statistics. (2004). Occupational Outlook Handbook: Registered Nurses
- ↑ NIH: Office of Science Education. (2006). [1] Advance News Magazines.(2005).
- ↑ Lifeworks: Art Therapist. URL accessed on 2007-02-17.
- ↑ Kerewsky, Shoshana. (2000). Beyond Internship: Helpful Resources for Obtaining Licensure.
- ↑ American Association for Marriage and Family Therapy, Frequently Asked Questions on Marriage and Family Therapists
- ↑ National Board for Certified Counselors. URL accessed on 2007-02-17.
- ↑ 34.0 34.1 34.2 Groth-Marnat, G. (2003). Handbook of Psychological Assessment, 4th ed. Hoboken, NJ : John Wiley & Sons. ISBN 0-471-41979-6
- ↑ 35.0 35.1 Jablensky, Assen. (2005). Categories, dimensions and prototypes: Critical issues for psychiatric classification. Psychopathology, 38(4), 201
- ↑ 36.0 36.1 Widiger, Thomas & Trull, Timothy. (2007). Plate tectonics in the classification of personality disorder: shifting to a dimensional model. American Psychologist, 62(2), 71-83.
- ↑ Mundt, Christoph & Backenstrass, Matthias. (2005). Psychotherapy and classification: Psychological, psychodynamic, and cognitive aspects. Psychopathology, 38(4), 219
- ↑ Kinderman, P. and Lobban, F. (2000) Evolving formulations: Sharing complex information with clients. Behavioural and Cognitive Psychotherapy, 28(3), 307-310
- ↑ Keutzer, Carolin. (1984). Transpersonal psychotherapy: Reflections on the genre. Professional Psychology: Research and Practice, 15(6), 868
- ↑ 40.0 40.1 Gabbard, Glen. (2005). Psychodynamic Psychiatry in Clinical Practice, 4th Ed. Washington, DC : American Psychiatric Press. ISBN 1-58562-185-4
- ↑ Beck, A., Davis, D., and Freeman, A. (2007). Cognitive Therapy of Personality Disorders, 2nd Ed. New York : Guilford Press. ISBN 978-1-59385-476-8
- ↑ Association for Behavioral and Cognitive Therapies. (2006). What is CBT?. Retrieved 03-04-2007.
- ↑ Lynch, Thomas and Robins, Clive. (1997). Treatment of Borderline Personality Disorder Using Dialectical Behavior Therapy. The Journal, 8(1).
- ↑ McMillan, Michael. (2004). The Person-Centred Approach to Therapeutic Change. London, Thousand Oaks : SAGE Publications. ISBN 0761948686
- ↑ Rowan, John. (2001). Ordinary Ecstasy : The Dialectics of Humanistic Psychology. London, UK : Brunner-Routledge. ISBN 0415236339
- ↑ Bitter, J. & Corey, G. (2001). "Family Systems Therapy" in Gerald Corey (ed.), Theory and Practice of Counseling and Psychotherapy. Belmost, CA : Brooks/Cole.
- ↑ Van Deurzen, Emmy. (2002). Existential Counseling & Psychotherapy in Practice. London; Thousand Oaks : Sage Publications. ISBN 0761962239
- ↑ Woldt, Ansel and Toman, Sarah. (2005). Gestalt Therapy: History, Theory, and Practice. Thousand Oaks, CA. : Sage Publications. ISBN 0761927913
- ↑ Slife, B., Barlow, S. and Williams, R. (2001). Critical issues in psychotherapy : translating new ideas into practice. London : SAGE. ISBN 0761920803
- ↑ Blatner, Adam. (1997). The Implications of Postmodernism for Psychotherapy. Individual Psychology, 53(4), 476-482.
- ↑ Boorstein, Seymour. (1996). Transpersonal Psychotherapy. Albany : State University of New York Press. ISBN 0791428354
- ↑ Norcross, John and Goldfried, Marvin. (2005). The Future of Psychotherapy Integration: A Roundtable. Journal of Psychotherapy Integration, 15(4), 392
- ↑ La Roche, Martin. (2005). The cultural context and the psychotherapeutic process: Toward a culturally sensitive psychotherapy. Journal of Psychotherapy Integration, 15(2), 169–185
- ↑ Young, Mark. (2005). Learning the Art of Helping, 3rd ed. Ch. 4, "Helping Someone Who is Different." Upper Saddle River, NJ : Pearson Education. ISBN 013111753X
- ↑ Seligman, Martin and Csikszentmihalyi, Mihaly. (2000). Positive psychology: An introduction. American Psychologist, 55(1), 5-14.
- ↑ Snyder, C. and Lopez, S. (2001). Handbook of Positive Psychology. New York ; Oxford : Oxford University Press. ISBN 0195135334
- ↑ Linley, Alex, et al. (2006). Positive psychology: Past, present, and (possible) future. The Journal of Positive Psychology, 1(1), 3-16.
- ↑ Seligman, M., Rashid, T., & Parks, A. (2006). Positive Psychotherapy. American Psychologist, 61(8), 774-788.
- ↑ Hill, Marcia and Ballou, Mary. (2005). The foundation and future of feminist therapy. New York : Haworth Press. ISBN 0789002019
- ↑ International Society of Psychiatric-Mental Health Nurses. (2001). Response to Clinical Psychologists Prescribing Psychotropic Medications. URL accessed on 2007-03-03.
- ↑ Lilienfeld, Scott and Lynn, Steven and Lohr, Jeffrey. (2002). Science and Pseudoscience in Clinical Psychology. New York : Guilford Press. ISBN 1572308281
References & Bibliography
Key texts
Books
Papers
Additional material
Books
Papers
External links
External links
Organizations
- APA Society of Clinical Psychology (Division 12)
- American Academy of Clinical Psychology
- American Board of Professional Psychology
- American Counseling Association
- American Association for Marriage and Family Therapy
- Association of State and Provincial Psychology Boards (ASPPB)
- Society for the Exploration of Psychotherapy Integration
- National Institute of Mental Health
Information
- Info on the field of psychology form the U.S. Department of Labor, Bureau of Labor Statistics
- The Psychology Wiki
- Classics in the History of Psychology
- All About Psychotherapy
Career and Education
- Careers in Psychology
- Careers in Clinical and Counseling Psychology
- Graduate School Programs in Clinical Psychology
- APA Accredited Programs in Clinical Psychology
- Getting into Graduate School, APA
International
- International Society of Clinical Psychology
- International PSY Congresses
- Canadian Psychological Society
- British Psychological Society
- Psychology Societies Outside the U.S.
Finding a therapist
- Find A Psychologist, APA
- Find A Therapist, Psychology Today
- TherapistLocator.net, American Association for Marriage and Family Therapy
| This page uses Creative Commons Licensed content from Wikipedia (view authors). |